Keynote: The nationwide NHS roll-out of AI-derived FFR-CT for patients with suspected coronary artery disease was safe, reduced unnecessary invasive and non-invasive cardiac testing, improved the efficiency of the revascularisation pathway, and demonstrated equitable adoption across regions and populations.
Keywords: AI diagnostics, FFR-CT, coronary artery disease, CCTA, NHS, cardiovascular outcomes
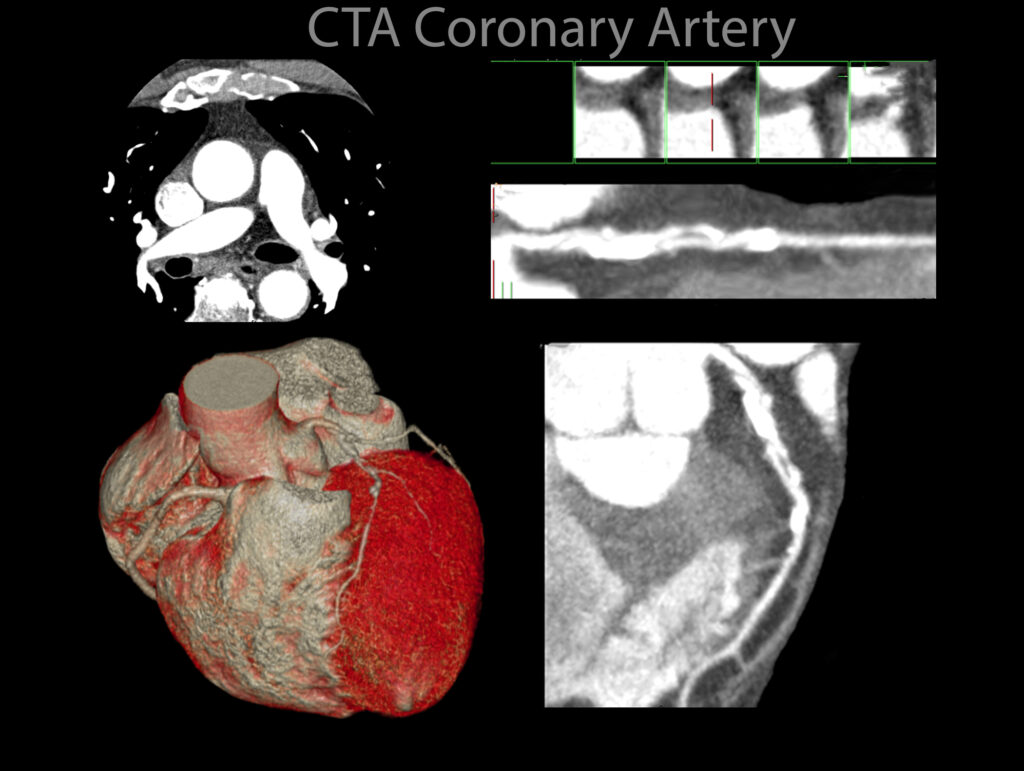
Artificial intelligence is transforming cardiovascular diagnostics in the NHS, and one of the most notable developments is the national implementation of AI-derived fractional flow reserve computed tomography (FFR-CT). This technology analyses coronary CT angiography (CCTA) scans to estimate blood flow through the coronary arteries, helping clinicians determine whether a patient with suspected coronary artery disease (CAD) requires further invasive testing or treatment.
A recent large-scale NHS evaluation across 27 hospitals has shown that this AI tool can be integrated safely into routine care, reduce unnecessary cardiac investigations, improve the efficiency of revascularisation pathways, and be adopted equitably across the UK.
What is FFR-CT and Why Does It Matter?
FFR-CT utilises advanced AI algorithms to model coronary blood flow from a standard CCTA scan, eliminating the need for an invasive catheter procedure. A fractional flow reserve value of 0.80 or below typically indicates that a coronary artery is significantly narrowed and may benefit from intervention. This non-invasive, AI-supported approach can spare patients from unnecessary invasive coronary angiography (ICA) and guide treatment more effectively.
The NHS Study: Scope and Scale
Between April 2017 and December 2020, NHS hospitals rolled out FFR-CT as part of the stable chest pain assessment pathway.
The evaluation covered over 102,000 CCTA examinations from 90,553 patients, of whom 54,865 were scanned after FFR-CT became available locally. Within this group, around 8.7% underwent FFR-CT analysis.
The follow-up period lasted a median of 1,211 days, with nearly all patients (98.1%) completing two years of monitoring.
Key Findings
Safety
The introduction of FFR-CT showed no increase in mortality risk. While unadjusted figures suggested lower death rates after the tool’s adoption, adjusted analyses showed similar rates for all-cause and cardiovascular mortality. The risk of myocardial infarction (MI) appeared slightly higher after adjustment; however, the authors caution that this could be due to confounding factors, changes in case mix, or the impact of the COVID-19 pandemic.
System Efficiency
One of the most significant benefits was the reduction of unnecessary testing.
- Invasive coronary angiography decreased by around 7%, with the most significant decrease observed in procedures that did not result in revascularisation.
- Non-invasive downstream testing (e.g., stress echocardiography, nuclear perfusion imaging) also declined, with a modest drop in repeat CCTA scans.
- The use of cardiac MRI and intracoronary imaging increased slightly, reflecting a targeted approach for more complex cases.
Importantly, among patients taken to the catheter lab, the proportion who went on to receive a revascularisation increased — an efficiency gain indicating fewer purely diagnostic procedures.
Prognostic Value
Within the FFR-CT subgroup, a positive result (≤0.80) strongly predicted worse outcomes over a two-year period. Compared to those with higher FFR-CT values, these patients were:
- Three times more likely to die from cardiovascular causes
- Five times more likely to have an MI
- Thirteen times more likely to undergo revascularisation
Adoption and Learning Curve
The programme scaled rapidly and evenly across different NHS regions and socio-economic groups, demonstrating equitable access. Over time, hospitals refined patient selection and reduced second-line testing, indicating a growing familiarity and confidence with the technology.
Strengths and Limitations
The study’s strengths lie in its nationwide scope, use of linked health records, and alignment with findings from previous randomised trials, which showed fewer unnecessary invasive angiograms. However, the observational design means residual confounding cannot be ruled out, and certain results may be influenced by time-period effects, particularly during the pandemic.
Looking Ahead
The NHS experience with AI-derived FFR-CT suggests it can safely support a CCTA-first strategy, streamline the diagnostic process, and improve the yield of invasive cardiac procedures. Future priorities include monitoring longer-term patient outcomes, analysing the specific mechanisms of post-adoption MI, and assessing cost-effectiveness in routine NHS practice.
Reference: Fairbairn, T.A., Mullen, L., Nicol, E. et al. Implementation of a national AI technology program on cardiovascular outcomes and the health system. Nat Med 31, 1903–1910 (2025). https://doi.org/10.1038/s41591-025-03620-y
Disclaimer: This article is an independent interpretation of the published study and is intended for educational purposes. It should not be used as a substitute for professional medical advice, diagnosis, or treatment.
home »