CASE REPORT
Finn Edler von Eyben1,*, Timo Joensuu2, Aki Kangasmaki2, Kalevi Kairemo2, Timo Kiljunen2
1Center of Tobacco Control Research, Odense, Denmark
2Docrates Cancer Center, Helsinki, Finland
Abstract
A 50-year-old man with prostate cancer was initially treated with radical prostatectomy and pelvic lymph node dissection. He had salvage androgen deprivation therapy (ADT) for persistent measurable prostate-specific antigen (PSA). In 2011, the first recurrence was treated with volumetric modulated arc therapy (VMAT). However, in 2014, an 11C-choline PET/CT scan indicated a second recurrence with new lesions, in two para-aortal lymph nodes. Abiraterone (Zytiga®) gave a fall of PSA from 2.9 to 0.54 ng/mL over four-month period. Following this, a para-aortal lymph node lesion was given VMAT with a boost of 60 Gy. The treatment was well tolerated.
Keywords: Abiraterone; external beam radiotherapy; PET/CT scanning; prostate cancer
1. Introduction
The main curative treatments of prostate cancer are radical prostatectomy (RP) or radical external beam radiotherapy (EBRT). For high-risk patients, a combination of first-line androgen deprivation therapy (ADT) and EBRT is better than treatment with only EBRT [1]. This first-line treatment of ADT includes the application of luteinizing-hormone-releasing hormone (LHRH) agonists or antagonists and/or anti-androgens, and surgery with bilateral orchiectomy. Nevertheless, one-third of these patients treated with radical prostatectomy (RP) or radical external beam radiotherapy (EBRT) have a recurrence of this condition.
Oncologists give salvage EBRT (SEBRT) with curative intent for patients with the first prostate-specific antigen (PSA) recurrence after RP [2]. In addition, oncologists rarely report treatment of second PSA recurrence. A few studies showed the effect of second-line SEBRT for patients with up to three lesions detected with PET/CT [3]. Another study showed the effect of steroid anti-androgens being changed to non-steroid antiandrogens [4]. Abiraterone is a second-line ADT. Abiraterone prolonged PSA recurrence-free survival for patients with metastatic prostate cancer who have failed with first-line ADT and chemotherapy [5].
We report a case with a second PSA recurrence of castrate-resistant prostate cancer. An 11C-choline PET/CT scan showed two new lesions in para-aortic lymph-nodes. The aim of this case report is to analyze the short-term efficacy and toxicity with abiraterone and volumetric-modulated arc therapy (VMAT).
2. Case report
In 2007, a 50-year-old man underwent RP and limited pelvic lymph node dissection for prostate cancer. The PSA level pretreatment was 18 ng/mL: pathology showed positive surgical margins, involvement of seminal vesicles, bilateral lymph node metastases, and a Gleason score of 9. The PSA did not fall to unmeasurable levels after the surgery. Therefore, he started salvage first-line ADT with bicalutamide and goserelin, followed with bilateral orchiectomy.
In the second quarter of 2009, the PSA became progressively increased. In June 2011, an 18F-fluorocyclobutane-1-carboxylic acid (18F-FACBC) PET/CT scan showed a lesion in a single pelvic lymph node. The patient underwent VMAT for the recurrent disease and obtained a partial remission for a period of 16 months [6]. In the third quarter of 2012, he had a new rise of PSA. The increase from May 2013 to May 2014 resulted in a decrease in PSA doubling time to 4 months and a PSA velocity increasing to 2.5 ng/mL/year, as shown in Figure 1.
In the fourth quarter of 2013, initial restaging with technetium-99m bone scan and an 18F-NaF PET/CT scan was negative. In contrast, an 11C-choline PET/CT showed a second recurrence, with two new lesions in para-aortic lymph nodes in March 2014. Consequently, he started abiraterone treatment in March 2014 and obtained a reduction in PSA from 2.9 to 0.54 ng/mL within the following four months.
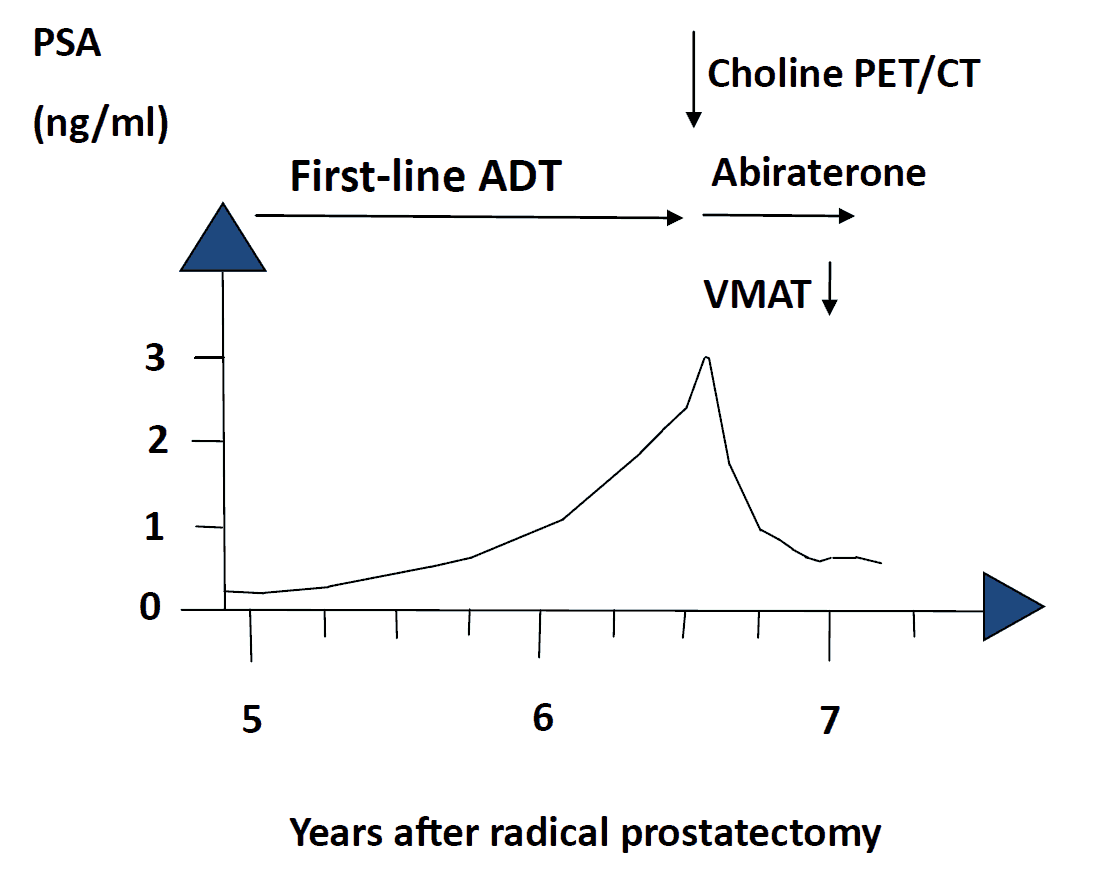
Figure 1. The PSA level increased before the start of treatment with abiraterone and declined after treatment. VMAT denotes volumetric modulated arc therapy.
The para-aortic lymph nodes were treated with VMAT from June to July 2014. The 11C-choline PET/CT scan was fused with the dose planning CT, and gross tumor volume (GTV) was based on the 11C-choline PET/CT findings, as shown in Figure 2.
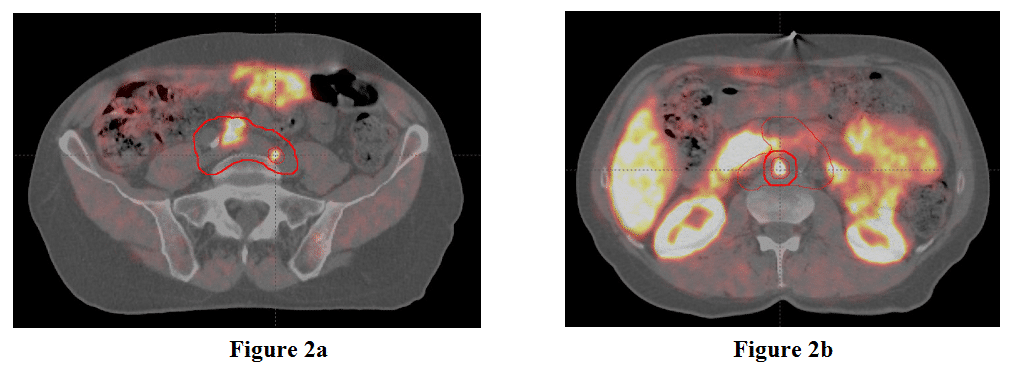
Figure 2. The caudal gross tumor volume (Figure 2a), and cranial gross tumor volume and the planned treatment volume boost, (Figure 2b). The para-aortic lymph node planned treatment volume (a, b) are presented in (Figure 2 a,b) where 11C-choline PET/CT is registered with CT simulation image.
The caudal GTV was 1.1 cm3 and the cranial GTV was 5.9 cm3. The planned treatment volume (PTV) for the para-aortic lymph nodes was 545 cm3. The cranial PTV included the GTV with a 5 mm margin. Figure 3 shows the dose planning summary for PTV for the lymph nodes.
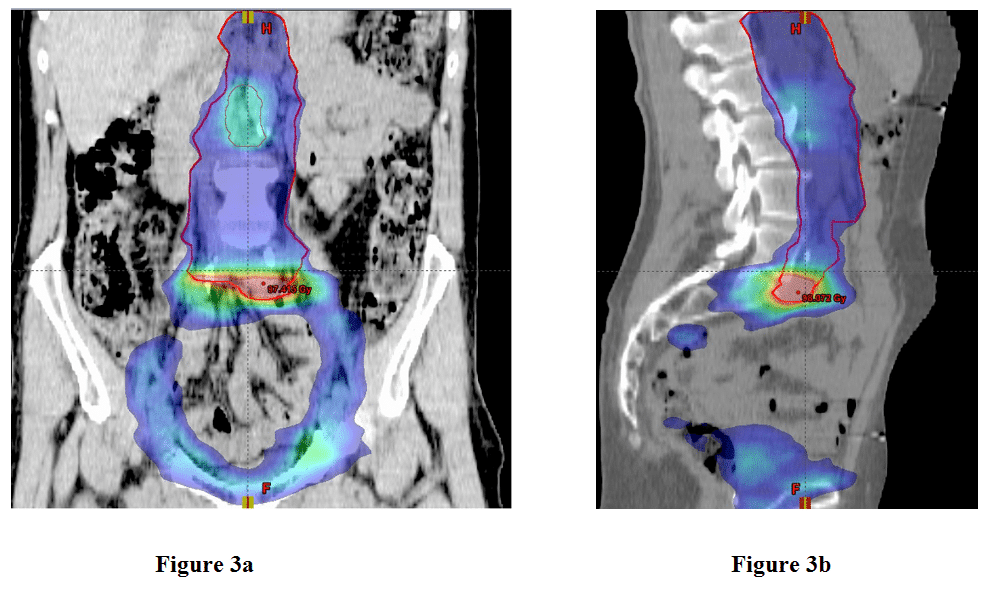
Figure 3. The coronal (a) and sagittal (b) dose distribution for the lymph nodes ranged from 44 to 90 Gy for the total VMAT treatments during the years 2011 and 2014. Planned treatment volume for the new para-aortal lesions is shown as a solid red line.
We used the Varian Aria Eclipse 11.0 control system for treatment planning and a 6 MV photons Varian iX linear accelerator.
Constraints for the PTV implied:
(1) At least 95% of the prescribed dose should be given to at least 99% of the PTV;
(2) A maximum radiation dose should be 103% or less of the prescribed dose;
(3) Dose should be minimal to the surrounding healthy organs at risk, including intestines and corpora of lumbar spine.
The caudal GTV that was already partly treated in 2011 was repeated along with the para-aortic lymph nodes from L1 to L5 to a dose of 45 Gy, in 25 fractions of 1.8 Gy, during a period of 5 weeks. Due to the previous SEBRT, a small overlapping lymph node volume received 90 Gy as a sum dose (V90Gy = 22 cm3). The cranial PTV was treated as a simultaneous integrated boost (SIB) to 50 Gy during the first 5 weeks of treatment and then alone to 60 Gy during the 6th week.
The patient had no acute toxicities during SEBRT and no late toxicity during the next two months. Follow-up after VMAT showed grossly stable PSA levels until August of 2014. The patient has given consent to the treatment and to publication of this report.
3. Discussion
This case report has important points for recurrent oligometastatic prostate cancer:
(1) PET/CT detected the sites of PSA recurrence while PSA was low;
(2) Change from first-line ADT to abiraterone was based on the 11C -choline PET/CT;
(3) Treatment with abiraterone reduced PSA to a level less than 20%;
(4) The combined abiraterone acetate and VMAT treatment did not increase toxicity and did not cause a PSA flare. Unfortunately, during 2014, the PSA changed less after VMAT than after VMAT in 2011.
This case history reflects recent changes in management to active imaging and treatment of oligometastatic prostate cancer. In 2014, 11C-choline PET/CT scanning became a Danish precedent for restaging for selected patients. With a PSA recurrence <10 ng/mL in the patient, the bone scan was expected to be negative [7]. With a PSA level >1 ng/mg and the PSA kinetics with short PSA doubling time <6 months and a high PSA velocity >2 ng/mL, it was likely that an 11C-choline PET/CT would give positive findings [8]. Positive scans differentiate between local, regional, and distant lesions and influence treatment decision [7].
In a study by Casamassima et al. 11C-choline PET/CT detected lymph node lesions for 25 of 71 patients [9]. In a study by Ceci et al. 11C-choline PET/CT changed treatment for 46% of 150 patients [10].
The oncologist regarded the positive findings of the 11C-choline PET/CT scans as a second relapse of oligometastatic prostate cancer. Accordingly, treatment was commenced with abiraterone, due to the positive results of a trial of metastatic chemo naïve patients, published in 2013 [11]. The patient had a marked reduction of PSA after he started treatment with abiraterone. This is important for SEBRT. Patients who achieved a fall of PSA to <0.5 ng/mL following neoadjuvant ADT before the start of EBRT, had better PSA recurrence-free survival from EBRT, than patients with a more modest fall of PSA [12].
EBRT for the patient followed standard fractionation and cumulative radiation dose. Several studies point to a dose-response relationship between prostate cancer and radiotherapy [13]. In a study, a radiation dose above 80 Gy increased survival rates, than a lower radiation dose [14]. An ultrahigh radiation dose might be needed for tumor control, but an ultrahigh dose may also increase the dose in organs at risk and the overall toxicity.
To circumvent this problem, some studies used an ultra-high simultaneous integrated boost (SIB) dose for lesions detected with imaging systems such as MRI and PET/CT to limited damage to the surrounding organs [15]. Wurschmidt et al. treated PET/CT positive lesions in lymph nodes with 66.6 Gy [16]. However, in direct contrast, in the study by Casamassima et al. the lymph node lesions detected with an 11C-choline PET/CT scan, were treated with 50 Gy in 25 fractions plus 24 Gy in an additional boost [9]. Consequently, we could have increased the radiation dosages for our patient without having caused severe toxicity to the surrounding organs at risk.
Nevertheless, there are few previous studies of treatment for oligometastatic prostate cancer [17]. In one study, half the patients had a second PSA recurrence within four years after treatment of the first PSA recurrence. Today, oncologists treat many patients with first PSA recurrence according to present guidelines [2]. Therefore, there is a growing demand for guidelines for a second PSA recurrence.
This case report is the first combination of abiraterone and VMAT as a new treatment for patients with second recurrence of lymph-node positive prostate cancer. The case report is limited by not having a large patient group to be able to compare and evaluate the findings. There is an ongoing FLAME controlled trial, which compares the outcomes using a boost of 95 Gy to the intraprostatic dominant lesions which have been diagnosed with MRI imaging. This is compared to conventional dose EBRT for the whole prostate gland without guidance for PTV by imaging from MRI or PET/CT scanning [18].
The STOMP controlled trial investigates whether metastasis-directed treatment has an effect for patients with oligometastatic prostate cancer [19]. Several studies investigate the combination of abiraterone and EBRT (NCT01717053 and NCT01780220).
4. Conclusion
In conclusion, 11C-choline PET/CT restaging of a patient with second PSA recurrence was followed by an effective and well-tolerated treatment with abiraterone and VMAT.
Conflict of interest
The authors confirm that this article content has no conflict of interest.
Acknowledgement
The authors thank the patient for information regarding his treatment plan. The Docrates Cancer Center, Helsinki, Finland, performed the VMAT in the para-aortic lymph nodes for the patient.
References
Key References: 1, 3, 4, 6, 7, 9, 11, 12, 17,19
- Zumsteg ZS, Spratt DE, Pei X, et al. Short-term androgen-deprivation therapy improves prostate cancer-specific mortality in intermediate-risk prostate cancer patients undergoing dose-escalated external beam radiation therapy. Int J Radiat Oncol Biol Phys. 2013; 85: 1012-1017. [CrossRef] [PubMed Abstract]
- Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer. Part II: Treatment of advanced, relapsing, and castration-resistant prostate cancer. Eur Urol. 2014; 65: 467-479. [CrossRef] [PubMed Abstract]
- Berkovic P, De Meerleer G, Delrue L, et al. Salvage stereotactic body radiotherapy for patients with limited prostate cancer metastases: deferring androgen deprivation therapy. Clin Genitourin Cancer. 2013; 11: 27-32. [CrossRef] [PubMed Abstract]
- Matsumoto K, Hagiwara M, Hayakawa N, et al. Third-line hormonal therapy to treat prostate cancer relapse after initial and second-line hormonal therapy: report of 52 cases and literature review. Asian Pac J Cancer Prev. 2014; 15: 3645-3649. [CrossRef] [PubMed Abstract]
- Fizazi K, Scher HI, Molina A, et al. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA-301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol. 2012; 13: 983-992. [CrossRef] [PubMed Abstract]
- von Eyben FE, Kangasmaki A, Kiljunen T, Joensuu T. Volumetric-modulated arc therapy for a pelvic lymph node metastasis from prostate cancer: a case report. Tumori. 2013; 99: e120-e123. [PubMed Abstract]
- von Eyben FE, Kairemo K. Meta-analysis of (11)C-choline and (18)F-choline PET/CT for management of patients with prostate cancer. Nucl Med Commun. 2014; 35: 221-230. [PubMed Abstract]
- Castellucci P, Ceci F, Graziani T, et al. Early Biochemical Relapse After Radical Prostatectomy: Which Prostate Cancer Patients May Benefit from a Restaging 11C-Choline PET/CT Scan Before Salvage Radiation Therapy? J Nucl Med. 2014; 55: 1424-1429. [CrossRef] [PubMed Abstract]
- Casamassima F, Masi L, Menichelli C, et al. Efficacy of eradicative radiotherapy for limited nodal metastases detected with choline PET scan in prostate cancer patients. Tumori. 2011; 97: 49-55. [PubMed Abstract]
- Ceci F, Herrmann K, Castellucci P, et al. Impact of C-choline PET/CT on clinical decision making in recurrent prostate cancer: results from a retrospective two-centre trial. Eur J Nucl Med Mol Imaging. 2014; Aug 15 (PMID:25182750). [PubMed Abstract]
- Ryan CJ, Smith MR, de Bono JS, et al. Abiraterone in metastatic prostate cancer without previous chemotherapy. N Engl J Med. 2013; 368: 138-148. [CrossRef] [PubMed Abstract]
- Zelefsky MJ, Gomez DR, Polkinghorn WR, Pei X, Kollmeier M. Biochemical response to androgen deprivation therapy before external beam radiation therapy predicts long-term prostate cancer survival outcomes. Int J Radiat Oncol Biol Phys. 2013; 86: 529-533. [CrossRef] [PubMed Abstract]
- Nomiya T, Tsuji H, Toyama S, et al. Management of high-risk prostate cancer: radiation therapy and hormonal therapy. Cancer Treat Rev. 2013; 39: 872-878. [CrossRef] [PubMed Abstract]
- Zelefsky MJ, Pei X, Chou JF, et al. Dose escalation for prostate cancer radiotherapy: predictors of long-term biochemical tumor control and distant metastases-free survival outcomes. Eur Urol. 2011; 60: 1133-1139. [CrossRef] [PubMed Abstract]
- Pinkawa M, Holy R, Piroth MD, et al. Intensity-modulated radiotherapy for prostate cancer implementing molecular imaging with 18F-choline PET-CT to define a simultaneous integrated boost. Strahlenther Onkol. 2010; 186: 600-606. [CrossRef] [PubMed Abstract]
- Wurschmidt F, Petersen C, Wahl A, Dahle J, Kretschmer M. [18F]fluoroethylcholine-PET/CT imaging for radiation treatment planning of recurrent and primary prostate cancer with dose escalation to PET/CT-positive lymph nodes. Radiat Oncol. 2011; 6: 44. [CrossRef] [PubMed Abstract]
- Schick U, Jorcano S, Nouet P, et al. Androgen deprivation and high-dose radiotherapy for oligometastatic prostate cancer patients with less than five regional and/or distant metastases. Acta Oncol. 2013; 52: 1622-1628. [CrossRef] [PubMed Abstract]
- Lips IM, van der Heide UA, Haustermans K, et al. Single blind randomized phase III trial to investigate the benefit of a focal lesion ablative microboost in prostate cancer (FLAME-trial): study protocol for a randomized controlled trial. Trials. 2011; 12: 255. [CrossRef] [PubMed Abstract]
- Decaestecker K, De Meerleer G, Ameye F, et al. Surveillance or metastasis-directed Therapy for OligoMetastatic Prostate cancer recurrence (STOMP): study protocol for a randomized phase II trial. BMC Cancer. 2014; 14: 671. [CrossRef] [PubMed Abstract]
Article information
Corresponding Author: Finn Edler von Eyben.
Copyright: © 2014 von Eyben FE et al.
How to cite: von Eyben FE, Joensuu T, Kangasmaki A, Kairemo K, Kiljunen T. Abiraterone and volumetric modulated arc therapy for second recurrence of node-positive prostate cancer – a case report. J. Diagn. Imaging Ther. 2014; 1(1): 73-80 (https://dx.doi.org/10.17229/jdit.2014-1028-005).
Article history: Received 03 October 2014; Revised 28 October 2014; Accepted 30 October 2014; Published online 30 October 2014.
Archive link: JDIT-2014-1028-005
home »