Positron Emission Tomography (PET) is a powerful medical imaging technique that provides detailed information about how tissues and organs function. Unlike traditional imaging methods that focus mainly on anatomy, PET reveals biochemical and physiological changes, often before any structural alterations become visible.
The process involves the use of radiotracers – molecules labelled with positron-emitting isotopes – which are introduced into the body, usually via injection. These tracers are designed to mimic or interact with natural compounds such as glucose, allowing them to participate in specific biological processes. When the tracer’s positrons encounter electrons in the body, they annihilate and produce gamma photons. PET scanners detect these photons and use advanced algorithms to reconstruct precise three-dimensional images showing where the tracer has accumulated.
PET is widely used in oncology to detect cancer, assess its spread, and monitor treatment response. In neurology, it helps investigate brain disorders such as Alzheimer’s disease, Parkinson’s disease, and epilepsy. In cardiology, PET can evaluate blood flow to the heart and determine whether damaged tissue is still viable.
By providing insight into the body’s inner workings at a molecular level, PET imaging plays a crucial role in early diagnosis, guiding treatment strategies, and advancing medical research.
Watch the Video: PET Imaging from Isotope to Diagnosis
This training scenario takes place at the Oncology Centre, where PET is routinely used for cancer staging, cardiac assessment, and neurological evaluation. By following the journey of a patient referred for a PET scan, you will see how isotopes are produced, how images are acquired, what technical challenges can arise, and why PET is often combined with CT or MRI.
At the end of this scenario, you will complete a Knowledge Check Quiz to test your understanding of PET imaging principles and clinical applications.
Scenario: James’ PET-CT Scan
Referral for PET
James, a 58-year-old man with suspected lung cancer, was referred for a PET-CT scan. The oncologist wanted to assess both the anatomical location of the lesion and its metabolic activity.
The nuclear medicine technologist explained that PET imaging is most commonly performed with Fluorine-18 labelled fluorodeoxyglucose (18F-FDG). This tracer mimics glucose and is taken up by cells in proportion to their metabolic activity. Because tumours often have high glucose metabolism, they appear as regions of increased uptake on PET images.
Radiopharmaceuticals and isotopes
The PET radiopharmaceutical used in James’ scan was 18F-FDG. Fluorine-18 is produced in a cyclotron, a type of particle accelerator that bombards oxygen-18 enriched water with protons. The resulting 18F has a half-life of about 110 minutes, making it suitable for regional distribution to imaging centres.
The technologist also mentioned that some isotopes used in PET emit both gamma and beta particles — for example, iodine-131 — but these are typically used for therapy rather than routine PET imaging. In PET, the key emission of interest is the positron (β+), which annihilates with an electron to produce two 511 keV gamma photons detected by the scanner.
Physics of PET
When a positron collides with an electron, they undergo annihilation, producing two gamma photons travelling in nearly opposite directions. PET scanners are ring-shaped detectors that capture these paired photons in coincidence detection. This allows reconstruction of the original site of annihilation, giving a 3D map of tracer distribution.
Because PET measures glucose uptake, the scan essentially provides an image of metabolic activity in tissues.
PET combined with CT or MRI
At the Oncology Centre, the PET scanner is integrated with a CT system. The CT provides precise anatomical localisation of the FDG uptake and is also used for attenuation correction, which compensates for photon absorption within the body. Without this correction, lesions in deep tissues could appear artificially less intense.
The physicist explained that PET-MRI systems do exist, but are less common than PET-CT. This is due to higher cost, longer acquisition times, and the complexity of integrating MRI hardware with PET detectors.
Artefacts and image quality
During James’ scan, the team stressed the importance of remaining still. Patient movement can lead to misalignment between PET and CT datasets, causing artefacts that complicate interpretation. Other sources of false findings include inflammation, infection, or high physiological uptake (such as in the brain, heart, or bladder). These can sometimes lead to false-positive results, so clinical context is essential.
Clinical applications
PET is used beyond oncology. In cardiology, PET can assess myocardial perfusion and viability, helping clinicians decide whether revascularisation would benefit the patient. In neurology, PET supports diagnosis of conditions such as Alzheimer’s disease by measuring brain metabolism.
The key advantage of PET over other imaging modalities is its ability to show functional and metabolic information, rather than just structural detail. This complements anatomical imaging and provides critical insights for personalised treatment planning.
Limitations of PET
The nuclear medicine physician reminded James that PET does have limitations. The spatial resolution is lower than CT or MRI, meaning very small lesions may be missed. In addition, PET scans expose patients to ionising radiation from both the radiopharmaceutical and the CT component. These risks are carefully managed by following the principle of ALARA (As Low As Reasonably Achievable).
Artefacts and attenuation correction in action
After the injection of 18F-FDG, James rested quietly for about an hour to allow tracer uptake. He was asked to avoid physical activity, since muscle movement could increase FDG uptake and mimic disease.
During the scan, the CT images were acquired first, followed by PET. The CT dataset was then used for attenuation correction, ensuring that deep lesions in the thorax and abdomen were not underestimated due to tissue absorption.
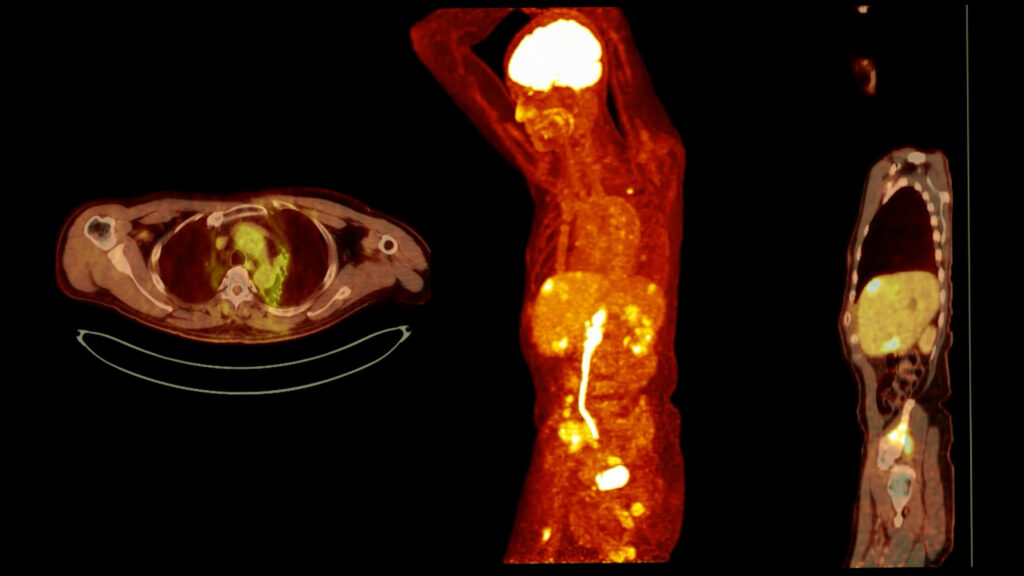
Image review
The resulting PET-CT images showed a metabolically active lesion in the left lung with associated lymph node uptake. The oncologist explained that the lungs typically show high uptake of oxygen but not FDG, so focal uptake in pulmonary tissue is considered suspicious. By contrast, the brain and bladder normally appear very bright due to high baseline glucose metabolism and urinary tracer excretion, respectively.
PET workflow summary
Through James’ case, several key PET principles were reinforced:
- PET stands for Positron Emission Tomography.
- The most commonly used radionuclide is 18F, typically in the form of FDG.
- The half-life of 18F is about 110 minutes.
- PET detects paired 511 keV photons following positron–electron annihilation.
- PET-CT is more common than PET-MRI because of cost and technical challenges.
- Patient movement causes artefacts that reduce diagnostic quality.
- PET’s main limitation is relatively poor spatial resolution.
- In cardiology, PET is used for perfusion and viability studies.
- The primary purpose of PET is to assess metabolic function.
- Attenuation correction is critical for quantitative accuracy.
Conclusion
James’ PET-CT case illustrates how radiopharmaceutical production, physics, and clinical applications come together in practice. PET provides unique insights into the functional status of tissues, supporting cancer staging, cardiac decision-making, and neurological assessment.
Although PET has limitations such as artefacts, false positives, and relatively low resolution, its ability to measure metabolic activity makes it an indispensable tool in modern medicine. When combined with CT or MRI, PET delivers both functional and anatomical information, enabling precise diagnosis and treatment planning.
Knowledge Check
You have now reviewed the essential principles of PET imaging through a clinical scenario. The following knowledge check quiz will test your understanding of isotopes, physics, artefacts, attenuation correction, clinical applications, and limitations of PET.
Instruction: Select the best answer from the options provided. Refer back to the scenario if needed, and use it to guide your responses. Completing the quiz will help consolidate your knowledge and prepare you for applying PET principles in clinical practice.
Disclaimer
This training scenario is provided for educational purposes only. It has been developed to illustrate the principles, physics, and clinical applications of PET imaging within a fictional case example.
The content does not replace professional medical training, institutional protocols, or regulatory guidance. Qualified healthcare professionals must make all clinical decisions regarding PET imaging and patient care in accordance with established standards, safety regulations, and institutional policies.
Any patients, hospitals, or cases described are fictional and included solely to support learning objectives.
Learners are reminded to always follow the ALARA principle, adhere to national and international radiation safety guidelines, and consult accredited professional resources when applying PET imaging concepts in practice.
home »