Radiolabelled peptides have already changed how we image and treat cancer, particularly through somatostatin receptor–targeted PET imaging and peptide receptor radionuclide therapy (PRRT). Over the last few years, though, the field has widened dramatically. New peptide targets, alpha-emitting radionuclides, smarter chelators and even peptide-based biomaterials are pushing radiopharmacy and nuclear medicine into a new phase.
This article walks through some of the most interesting recent developments, with an eye on what they mean in practice for imaging scientists, radiochemists, clinicians and anyone watching theranostics evolve in real time.
Beyond Somatostatin: A Broader Set of Peptide Targets
For a long time, radiolabelled peptide work was dominated by somatostatin analogues such as DOTATATE and DOTATOC, labelled with 68Ga for PET and 177Lu or 90Y for therapy. Those agents are now well established and integrated into clinical pathways. Current research is focused on expanding the menu of targets, especially in areas where conventional receptor-targeted approaches have been less effective.
Fibroblast Activation Protein (FAP): Targeting the Tumour Microenvironment
Fibroblast activation protein (FAP) has emerged as a particularly attractive target because it is expressed not on the cancer cells themselves but on cancer-associated fibroblasts within the tumour stroma. This opens the door to attacking the supporting infrastructure that tumours rely on.
FAP-2286 is a lead candidate in this area. It is a peptide conjugated to DOTA that can be labelled with 68Ga for PET imaging or 177Lu for therapy. Early clinical studies have shown high uptake across a range of solid tumours, with sustained retention, suggesting promising therapeutic applications. Centres are now fine-tuning automated 68Ga labelling protocols for routine production under GMP conditions, a critical step on the path to wider adoption.
Second-generation variants of FAP-2286 are also in development. Some incorporate structural modifications such as squaric acid linkers to improve tumour retention and optimise the balance between efficacy and off-target dose. The overall trend is clear: FAP-targeted peptides are well on their way to becoming a major new family of theranostic agents.
PSMA-Targeted Peptides in Prostate Cancer
Prostate-specific membrane antigen (PSMA) has transformed nuclear oncology for prostate cancer, largely through small-molecule ligands like PSMA-11 and PSMA-617. Alongside these, peptide-based PSMA constructs are being explored, often with albumin-binding moieties to extend blood circulation time and increase tumour uptake.
There is also growing interest in pairing PSMA-targeted ligands with alpha emitters such as 225Ac or 212Pb as an alternative in patients who relapse after 177Lu-PSMA therapy. These combinations are still in various stages of clinical and preclinical evaluation, but they fit into a broader move towards alpha therapy in resistant or advanced disease.
GRPR and Hormone Receptor Peptides
Gastrin-releasing peptide receptor (GRPR)-targeted peptides, including RM26 analogues, are being refined for both imaging and therapy in prostate, breast and other cancers. Small changes in linkers and chelators have led to improved metabolic stability and clearer in vivo targeting, with labelling demonstrated for radionuclides such as 99mTc and 68Ga.
Other hormone-related peptides, including analogues of luteinising hormone-releasing hormone (LHRH) and follicle-stimulating hormone (FSH), are under investigation as radionuclide carriers or as components of hybrid nanoparticle systems. These are at earlier stages but illustrate the trend towards exploiting endocrine pathways in a much more systematic way.
From Beta to Alpha: A New Generation of Peptide Therapies
Most established radiolabelled peptide therapies use beta emitters such as 177Lu or 90Y. These provide relatively long path lengths and a well-understood toxicity profile. However, as more patients relapse or develop resistance after β−PRRT, attention has turned to alpha emitters.
Why Alpha Emitters Are So Attractive
Alpha particles deliver a much higher linear energy transfer (LET) over a very short path length. That combination can cause dense, irreversible DNA damage in targeted cells while sparing surrounding tissue, provided the targeting vector is specific, and the radionuclide remains bound.
Peptide-based alpha therapies aim to harness this by simply swapping the radionuclide on a known peptide scaffold. For example, somatostatin analogues and PSMA ligands that already have a rich clinical evidence base with 177Lu can be relabelled with 225Ac or 212Pb. Early data suggest that such agents can induce responses in tumours that have progressed following conventional β−therapies.
Lead–Isotope Theranostic Pairs
212Pb is gaining particular attention as a short-lived in vivo generator of 212Bi, an alpha emitter, while 203Pb can serve as an imaging partner for SPECT-based dosimetry. This creates a matched theranostic pair, conceptually similar to 68Ga/177Lu in the PET setting, but tuned for alpha therapy.
Work with Pb-based systems underlines a broader shift towards precise dosimetry. Imaging and therapy doses are being more closely linked, with quantitative SPECT or PET used to inform patient-specific treatment planning and cumulative dose limits, particularly for the kidney and bone marrow.
Safety and Long-Term Effects
The appeal of alpha therapy is obvious, but questions remain. Myelosuppression, nephrotoxicity and the risk of late effects, such as secondary malignancies, require careful monitoring. Trial designs increasingly incorporate extended follow-up and detailed dosimetric endpoints. For now, many centres view alpha-labelled peptides as part of salvage regimens after β−PRRT, but there is a serious conversation about moving them earlier in the treatment sequence once long-term safety is better characterised.
Smarter Radiochemistry: Chelators, Generators and Automation
Clinical success with new peptides depends as much on radiochemistry and logistics as on biology. There has been significant progress in all three.
Optimising Chelators and Linkers
The classic macrocyclic chelators such as DOTA and NOTA remain central, but there is an active search for alternatives better suited to specific radionuclides, especially alpha emitters. The ideal chelator must form a complex that is both kinetically inert and stable in vivo under challenging conditions.
Parallel work on linkers is just as important. Linkers influence pharmacokinetics, receptor binding, internalisation and overall biodistribution. Small modifications can shift a peptide from rapid renal clearance to prolonged tumour retention. Current research is systematically exploring linker libraries and structure–activity relationships, aided by faster radiosynthesis and high-throughput screening.
Generator-Based Theranostic Platforms
From a practical standpoint, generator-based radionuclides are very appealing for hospitals without on-site cyclotrons. Recent work from UK groups has produced theranostic platforms built around 99mTc/188Re generator pairs and novel diphosphine chelators. These systems allow a wide range of peptides to be attached to the same scaffold, enabling SPECT imaging with 99mTc and β−therapy with 188Re.
The concept mirrors PET/PRRT theranostics but is tailored to sites where SPECT remains the main workhorse. Such platforms could widen access to peptide-based theranostics globally, especially in settings with constrained infrastructure.
Automation and GMP-Ready Protocols
Fully automated synthesis modules are now standard in many PET and therapy facilities, but newer peptides and radionuclides need dedicated optimisation. Research groups are publishing detailed 68Ga labelling protocols for experimental peptides such as FAP-2286, including reaction conditions, purification steps and quality control parameters suitable for GMP validation.
Automation does more than save staff time. It improves reproducibility across centres, simplifies multi-site trials and makes it easier for regulators to evaluate production processes. As more peptides progress from first-in-human studies to phase II and III trials, robust automated methods will become a prerequisite.
Peptides Meet Biomaterials and Nanotechnology
Another area gaining momentum is the integration of radiolabelled peptides with advanced biomaterials. Rather than using a single peptide as the sole targeting vector, researchers are building multi-component systems in which peptides are one part of a larger construct.
Self-Assembling Peptides and Hydrogels
Self-assembling peptide systems can form nanofibres or hydrogels in situ. When combined with radionuclides, these materials can act as local depots for sustained delivery, potentially useful for intratumoural or cavity-based therapy. The idea is to maintain a high local dose while reducing systemic exposure.
These concepts are still mainly preclinical, but they align with broader interest in localised radionuclide therapy, such as intracavitary applications in glioma or post-surgical settings.
Nanoparticles and Multimodal Agents
Nanoparticles incorporating radiolabelled peptides at the surface are being designed for combined imaging and therapy or for combination regimens with drugs, photothermal therapy or immunomodulators. Peptides provide the specificity, while the core offers additional functions such as drug loading or MRI contrast.
Although regulatory pathways for nanomedicines remain complex, these platforms highlight how peptide targeting can be blended with other treatment modalities. Over the next decade, it would not be surprising to see radiolabelled peptides used as part of multi-arm strategies rather than stand-alone agents in some indications.
Clinical and Service Implications
Taken together, these technical advances are already changing the questions clinicians and service planners must address.
In the clinic, there is a shift from asking “Do we have a peptide for this tumour type?” to “Which target, radionuclide and dosing strategy is most appropriate for this individual patient?” The growth of alpha therapy and microenvironment targets, such as FAP and hormone receptor peptides, is pushing practice towards more tailored regimens.
For imaging and therapy services, it raises issues such as:
- How to organise production when multiple peptide agents and radionuclides are in routine use.
- How to integrate quantitative imaging and dosimetry into day-to-day workflows, rather than keeping them as research extras.
- How to educate referring clinicians about the strengths and limitations of newer agents so that patient selection is realistic and evidence-based.
For radiochemists, the focus is shifting towards modular, scalable platforms that can be adapted quickly when new targets are validated, and towards generators and kits that lower barriers to adoption in smaller centres.
Looking Ahead
Radiolabelled peptides have already proved their worth in neuroendocrine tumours and prostate cancer. The recent wave of developments suggests that we are moving towards a much more diverse toolbox, where microenvironment targets, alpha emitters, generator-based platforms and peptide–material hybrids sit alongside the classics.
In the near term, wider access to FAP-targeted and PSMA-related theranostics and a gradual integration of alpha-labelled peptides into salvage and then front-line regimens seem very likely. Over a slightly longer horizon, the integration of radiolabelled peptides with biomaterials and nanoparticles may open new routes for localised and combination therapies.
For anyone involved in diagnostic imaging, nuclear medicine or radiopharmacy, it is an exciting time. The core principle remains the same—using small, highly specific peptides to carry radiation exactly where it is needed—but the tools are becoming more powerful, more adaptable and more closely linked to individual patient biology.
Radiolabelled Peptides — Expert Q&A Companion
What are radiolabelled peptides, and how are they used in modern oncology?
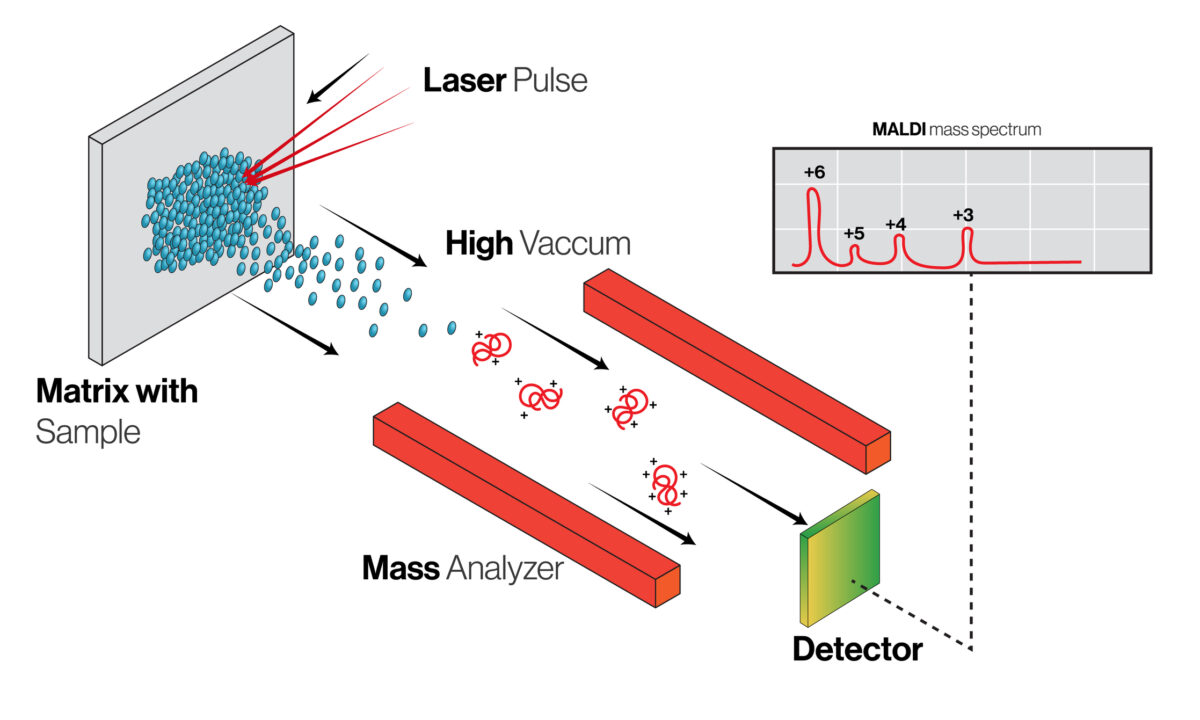
Radiolabelled peptides are short chains of amino acids linked to radioactive isotopes. Because they bind to specific biological targets that are over-expressed in tumours or their surrounding stroma, they can be used either for molecular imaging or for targeted radionuclide therapy. In imaging, they support PET or SPECT visualisation of disease. In therapy, they deliver radiation directly to cancer cells or tumour-associated structures, forming the basis of peptide receptor radionuclide therapy (PRRT).
How has the field evolved beyond traditional somatostatin-based therapies?
Somatostatin receptor ligands such as DOTATATE established the clinical value of radiolabelled peptides, particularly in neuroendocrine tumours. Current research is extending this approach to new biological targets, including tumour-associated fibroblasts, prostate-specific membrane antigen (PSMA), gastrin-releasing peptide receptors (GRPR) and hormone-linked pathways. This shift is widening the therapeutic landscape and enabling the development of disease-specific theranostic strategies.
Why is fibroblast activation protein (FAP) such an important emerging target?
FAP is expressed on cancer-associated fibroblasts within the tumour microenvironment. Targeting this stromal compartment allows radiolabelled peptides such as FAP-2286 to interfere with supportive tissue structures rather than tumour cells alone. These agents can be labelled for both PET imaging and targeted radionuclide therapy, and early studies indicate strong tumour uptake with encouraging retention characteristics. Efforts are now focused on optimising chemistry, improving tumour residence time and refining manufacturing workflows for wider clinical uptake.
What progress is being made with PSMA-targeted peptide radiopharmaceuticals?
In prostate cancer, PSMA remains one of the most clinically productive molecular targets. Newer PSMA-directed peptide constructs are incorporating albumin-binding components to extend systemic circulation and enhance tumour uptake. At the same time, research programmes are investigating PSMA ligands paired with alpha-emitting radionuclides for patients who relapse following β-emitter therapy, supporting a potential escalation pathway in advanced disease.
Which other peptide-based targets are currently under investigation?
GRPR-targeted ligands are being refined for applications in prostate, breast and other cancers, with improved metabolic stability and receptor selectivity. Analogues of reproductive hormones such as LHRH and FSH are also being explored as radionuclide carriers or as elements within hybrid nanomedicine systems. Many of these developments remain early-stage, but they illustrate the breadth of biological pathways now being investigated.
Why is there growing interest in alpha-emitting radionuclides for peptide therapy?
Alpha emitters deliver high linear energy transfer over extremely short distances, creating dense DNA damage within targeted cells. When combined with accurate molecular targeting, this approach may help control tumours that do not respond sufficiently to β-emitter therapy. Peptides labelled with isotopes such as 225Ac and 212Pb are showing promise in both research and early clinical settings, particularly in salvage treatment scenarios.
What is the significance of lead-based theranostic isotope pairs?
Lead-based systems pair 212Pb for therapy with 203Pb for SPECT imaging and dosimetry. This enables quantitative imaging and patient-specific treatment planning using the same molecular scaffold. The approach supports more accurate assessment of absorbed dose to organs and tumours, encouraging a move towards personalised radionuclide therapy rather than fixed, protocol-driven dose schedules.
What safety considerations apply to next-generation peptide therapies?
Although early experience has been positive, careful monitoring remains essential. Areas under active evaluation include renal and marrow dose tolerance, cumulative exposure across treatment cycles and the potential for late toxicities. Many centres currently integrate alpha-labelled peptides into salvage or second-line pathways, with broader adoption likely as evidence from longer-term follow-up accumulates.
How is radiochemistry advancing to support translation into practice?
Progress is visible across three interconnected areas. First, new chelators and linker systems are being designed to improve in vivo stability and optimise pharmacokinetics for specific radionuclides. Second, generator-based isotope platforms such as 99mTc/188Re are enabling cost-effective theranostic production in centres without cyclotrons. Third, automated labelling and GMP-ready synthesis protocols are making it easier to standardise manufacturing across multi-centre clinical trials.
What role do biomaterials and nanotechnology play in future peptide-based radionuclide therapies?
Research is exploring peptide-integrated biomaterials such as self-assembling hydrogels and nanoparticle constructs. These platforms may allow sustained local delivery, multimodal therapy combinations or enhanced tumour retention. Although currently preclinical in most cases, they signal a shift towards more sophisticated delivery architectures that sit alongside conventional peptide radiopharmaceuticals.
What does all this mean for clinical services and patient pathways?
As the range of available agents grows, services will need to support multiple radionuclides, target classes and production workflows. Quantitative imaging and dosimetry are likely to become more routine, particularly where alpha therapy or multi-cycle regimens are used. Multidisciplinary decision-making and appropriate patient selection will be increasingly important as theranostics moves closer to personalised care models.
How is the field likely to develop over the coming years?
Broader clinical access to FAP- and PSMA-based theranostics, gradual expansion of alpha-labelled peptide therapies and continued growth in modular chemistry platforms all appear likely. Over time, radiolabelled peptides are expected to play a central role in precision oncology strategies, working alongside systemic therapies, molecular imaging and emerging biomaterial-based approaches.
Disclaimer
This article is provided for informational and educational purposes only and does not constitute medical, clinical, scientific, or professional advice. The content reflects current research and developments in radiolabelled peptides at the time of writing. Still, it should not be used to guide patient care, diagnosis, treatment decisions, or radiopharmaceutical practice. Readers should consult qualified healthcare professionals, regulatory guidance, and institutional protocols before applying any concepts discussed here in clinical or laboratory settings. The authors and publishers accept no responsibility for any actions taken based on the information presented in this article.
home » blog » radiolabelling »