Summary: The use of carbon-13 (¹³C) breath tests has become a vital tool in modern diagnostics, offering a safe, non-invasive, and highly specific method for assessing metabolic, gastrointestinal, hepatic, and bacterial functions. This article explores the historical development of ¹³C breath tests, from the theoretical underpinnings of stable isotope science to their widespread clinical application. Beginning with the early use of radioisotopes in medicine, the shift to non-radioactive carbon-13 isotopes marked a turning point in safety and accessibility. The article traces the scientific milestones, technological advancements, and expanding range of clinical indications that have defined the progress of ¹³C breath testing over the past five decades.
Keywords: carbon-13, stable isotope, breath test, diagnostic tool, gastrointestinal function, medical history.
The Origins of Breath Testing in Medicine
The idea of using breath as a diagnostic window into the human body dates back to ancient times. Physicians of antiquity would often smell the breath of their patients, detecting sweet, foul, or alcoholic odours as signs of internal disease. While rudimentary and subjective, this instinct laid the foundation for modern breath diagnostics.
In the 20th century, scientific advances allowed breath to be analysed quantitatively. The advent of spectroscopy, gas chromatography, and later mass spectrometry made it possible to detect specific compounds in exhaled air. By the mid-1900s, clinicians and researchers began exploring isotopes—both radioactive and stable—as markers to trace metabolic processes via breath analysis.
From Radioisotopes to Stable Isotopes
Early breath tests often used radioactive isotopes such as carbon-14 (¹⁴C). These tests involved administering a compound labelled with ¹⁴C and measuring the amount of radioactive carbon dioxide (¹⁴CO₂) exhaled after metabolism. While effective, the health risks associated with radioactivity, particularly in vulnerable populations like children and pregnant women, limited their routine use.
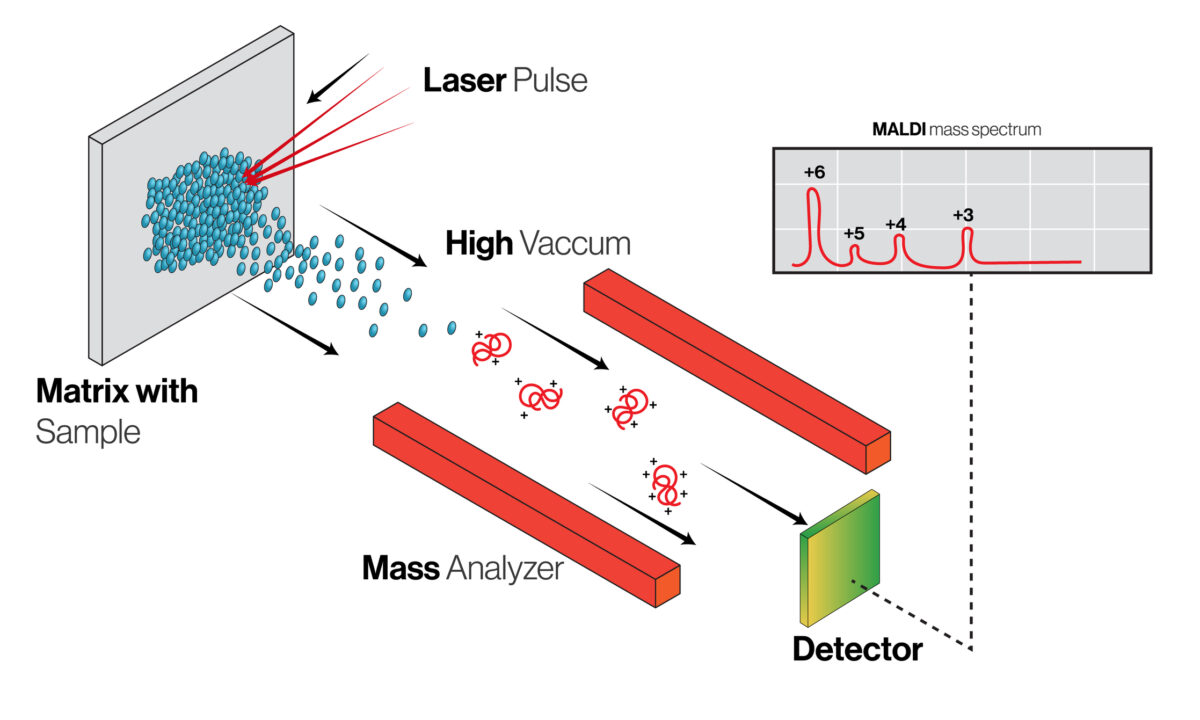
The discovery and application of stable isotopes changed this landscape. Carbon-13 (¹³C), a naturally occurring non-radioactive isotope of carbon, offered a safe and biologically identical alternative. Because it behaves the same as the more abundant carbon-12 (¹²C) in metabolic reactions, but can be distinguished using isotope ratio mass spectrometry (IRMS), ¹³C became the ideal tracer for breath tests.
The transition to ¹³C breath tests began in earnest during the 1970s. Researchers were motivated by the need for safer diagnostic tools, especially in areas such as paediatric hepatology, where liver function needed to be assessed without invasive procedures.
The First ¹³C Breath Tests
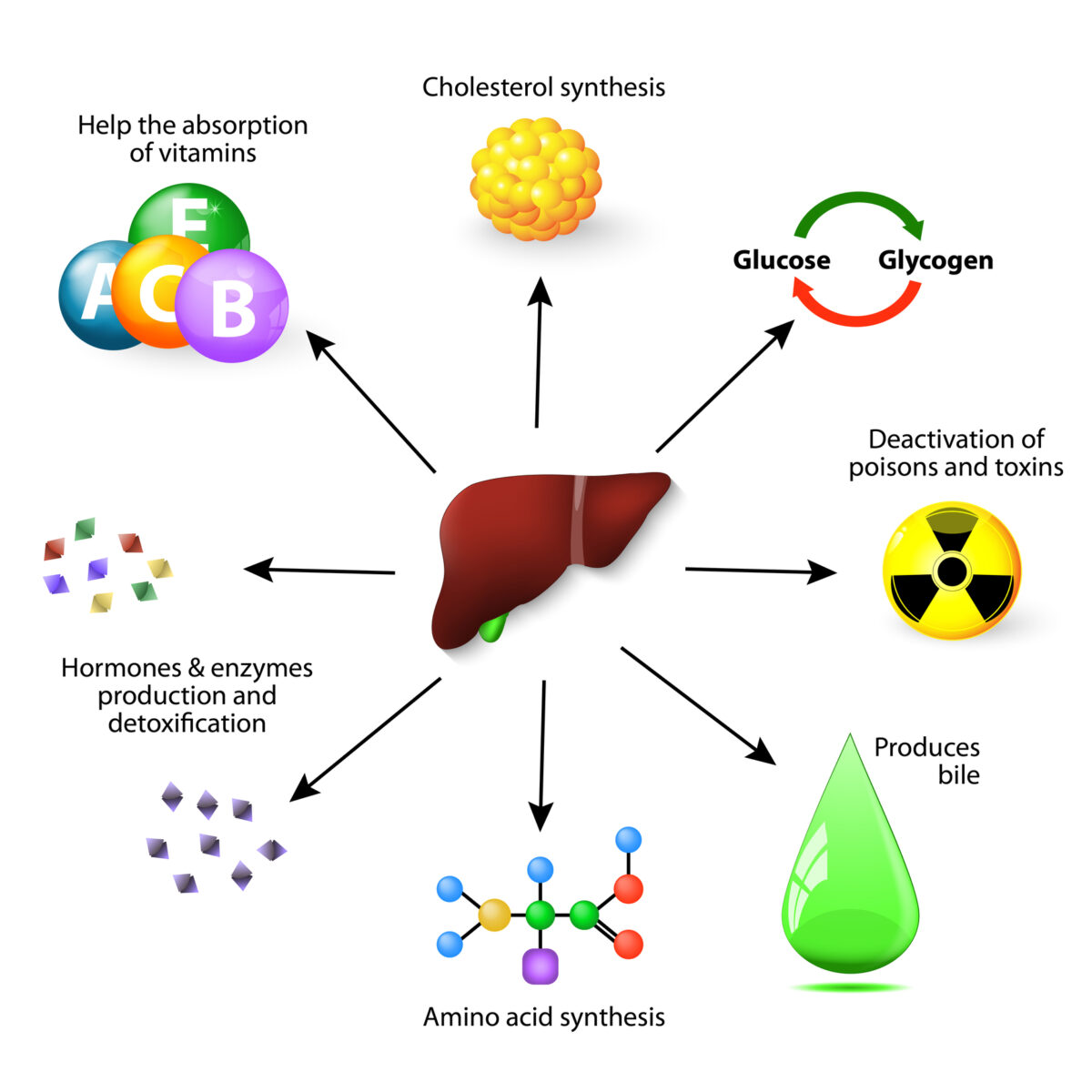
The first clinical applications of ¹³C-labelled compounds in breath testing focused on hepatic function. Compounds like ¹³C-methacetin and ¹³C-aminopyrine, metabolised primarily by liver enzymes, were administered orally or intravenously. The amount of ¹³CO₂ measured in the breath over time served as an indicator of hepatic enzyme activity, especially cytochrome P450 function. These tests were particularly useful in evaluating patients with liver cirrhosis, hepatitis, or suspected drug metabolism disorders.
By the 1980s, ¹³C-urea breath tests had emerged as a breakthrough for the detection of Helicobacter pylori, the bacterium associated with peptic ulcers and gastric cancer. Patients ingested ¹³C-labelled urea, and the presence of H. pylori led to its hydrolysis, producing labelled carbon dioxide that was detectable in the exhaled breath. This test provided a rapid, non-invasive alternative to endoscopic biopsy and culture, revolutionising the diagnosis and management of H. pylori infections.
Technological Advancements in Detection
The success of ¹³C breath testing depended not only on the isotopes themselves but also on the ability to detect them accurately and reliably. Early detection relied heavily on isotope ratio mass spectrometry (IRMS), which, while precise, was expensive, complex, and required specialised equipment.
Over time, technological improvements made breath analysis more accessible. Infrared spectroscopy, for instance, offered a simpler and faster method for detecting ¹³CO₂. Devices became portable, user-friendly, and cost-effective, enabling breath tests to transition from research laboratories to clinical settings. In some cases, breath test results could be obtained within minutes, facilitating point-of-care diagnostics.
The miniaturisation of devices and the development of automated analysers also made it easier to standardise tests across different healthcare environments. This was critical for ensuring the reproducibility and reliability of results, especially when comparing data across clinical trials or international studies.
Expanding Clinical Applications
Although initial breath tests focused on liver and gastric functions, subsequent research broadened their clinical scope. The ¹³C-octanoic acid breath test, for example, became an important tool for evaluating gastric emptying. Octanoic acid is a medium-chain fatty acid that, when labelled with ¹³C, is absorbed and metabolised rapidly, making it ideal for monitoring gastrointestinal motility.
Similarly, the ¹³C-phenylalanine and ¹³C-methionine breath tests allowed for the assessment of amino acid metabolism, particularly in inherited metabolic disorders. In cystic fibrosis, ¹³C-labelled fatty acid breath tests have helped evaluate pancreatic exocrine function.
More recently, ¹³C-labelled glucose and lactose breath tests have been employed to assess carbohydrate digestion and malabsorption, aiding in the diagnosis of conditions like lactose intolerance and small intestinal bacterial overgrowth (SIBO). These tests have found applications in both paediatric and adult populations, often replacing older, less specific hydrogen breath tests.
In hepatology, newer variations such as the ¹³C-ketoisocaproic acid breath test provide deeper insights into mitochondrial function and oxidative stress, demonstrating the continued innovation within this field.
Regulatory and Commercial Developments
As ¹³C breath testing grew in clinical relevance, commercial interest and regulatory scrutiny increased. In the 1990s and early 2000s, several companies began developing and marketing FDA- and CE-approved test kits. These kits standardised the test compounds, breath collection methods, and analytic protocols, improving consistency and encouraging adoption in routine clinical practice.
The urea breath test for H. pylori became the first to gain widespread regulatory approval and insurance reimbursement, setting the precedent for future breath tests. Public health agencies and professional societies began including breath tests in clinical guidelines, further legitimising their use.
In parallel, breath testing has been incorporated into clinical trials as a non-invasive biomarker for drug metabolism and liver function, especially in early-phase pharmacokinetics studies. The safety profile of ¹³C-labelled compounds makes them attractive in both healthy volunteer studies and vulnerable patient cohorts.
Challenges and Limitations
While ¹³C breath tests offer many advantages, they are not without limitations. Standardisation remains a concern across different test types, laboratories, and populations. Factors such as age, sex, body mass index, and diet can influence breath test results, necessitating robust reference ranges and interpretative algorithms.
Furthermore, breath test accuracy can be affected by recent food intake, physical activity, and gastrointestinal transit times. In some cases, false positives or negatives may occur due to overlapping pathologies or external contaminants.
Another challenge is accessibility. Although simplified infrared analysers have improved the situation, some breath tests still require laboratory-based analysis using IRMS, which may not be available in all healthcare settings, particularly in lower-income countries.
Nonetheless, ongoing research continues to refine test protocols, establish normative data, and explore new markers and metabolic pathways for future breath-based diagnostics.
The Future of ¹³C Breath Testing
As interest in personalised and non-invasive diagnostics grows, ¹³C breath tests are poised to play a more prominent role in medicine. Emerging areas include the use of breath tests to monitor disease progression or therapeutic response, particularly in chronic liver diseases and gastrointestinal motility disorders.
Artificial intelligence and machine learning are being applied to breath data to improve diagnostic accuracy and interpret complex metabolic patterns. Combined with wearable technology and remote data transmission, this could enable home-based breath testing for monitoring chronic conditions.
There is also increasing interest in combining ¹³C breath tests with other omics-based approaches, such as metabolomics or microbiome profiling, to gain a more holistic understanding of patient health.
New ¹³C-labelled compounds are in development for use in oncology, neurology, and endocrinology, suggesting that the clinical applications of this diagnostic method are far from exhausted.
Conclusion
The history of ¹³C breath testing reflects a broader shift in medicine towards safer, non-invasive, and patient-friendly diagnostic tools. From its early application in hepatology to its widespread use in diagnosing H. pylori and assessing gastrointestinal function, the ¹³C breath test has revolutionised clinical practice in multiple fields. Technological innovation, improved test design, and increasing integration into clinical guidelines have made it a reliable and versatile diagnostic option.
As the field continues to evolve, ¹³C breath testing holds promise not only for more accurate diagnostics but also for real-time disease monitoring and personalised care strategies. Its journey from laboratory curiosity to clinical mainstay underscores the power of stable isotope science in advancing modern healthcare.
Disclaimer
This article is intended for informational and educational purposes only. It does not constitute medical advice, diagnosis, or treatment, and should not be used as a substitute for professional medical guidance or clinical judgement. While every effort has been made to ensure the accuracy of the information presented, Open Medscience makes no representations or warranties, express or implied, regarding the completeness, accuracy, or reliability of the content.
Readers should consult qualified healthcare professionals before making decisions related to any medical condition, diagnostic test, or treatment method discussed herein. The historical and scientific content reflects current knowledge as of the date of publication and may evolve with future research and regulatory developments.
Any mention of specific tests, products, or technologies does not imply endorsement by Open Medscience. Open Medscience disclaims any liability for loss, injury, or damage resulting from the use of information contained in this article.
home » blog » radiolabelling »