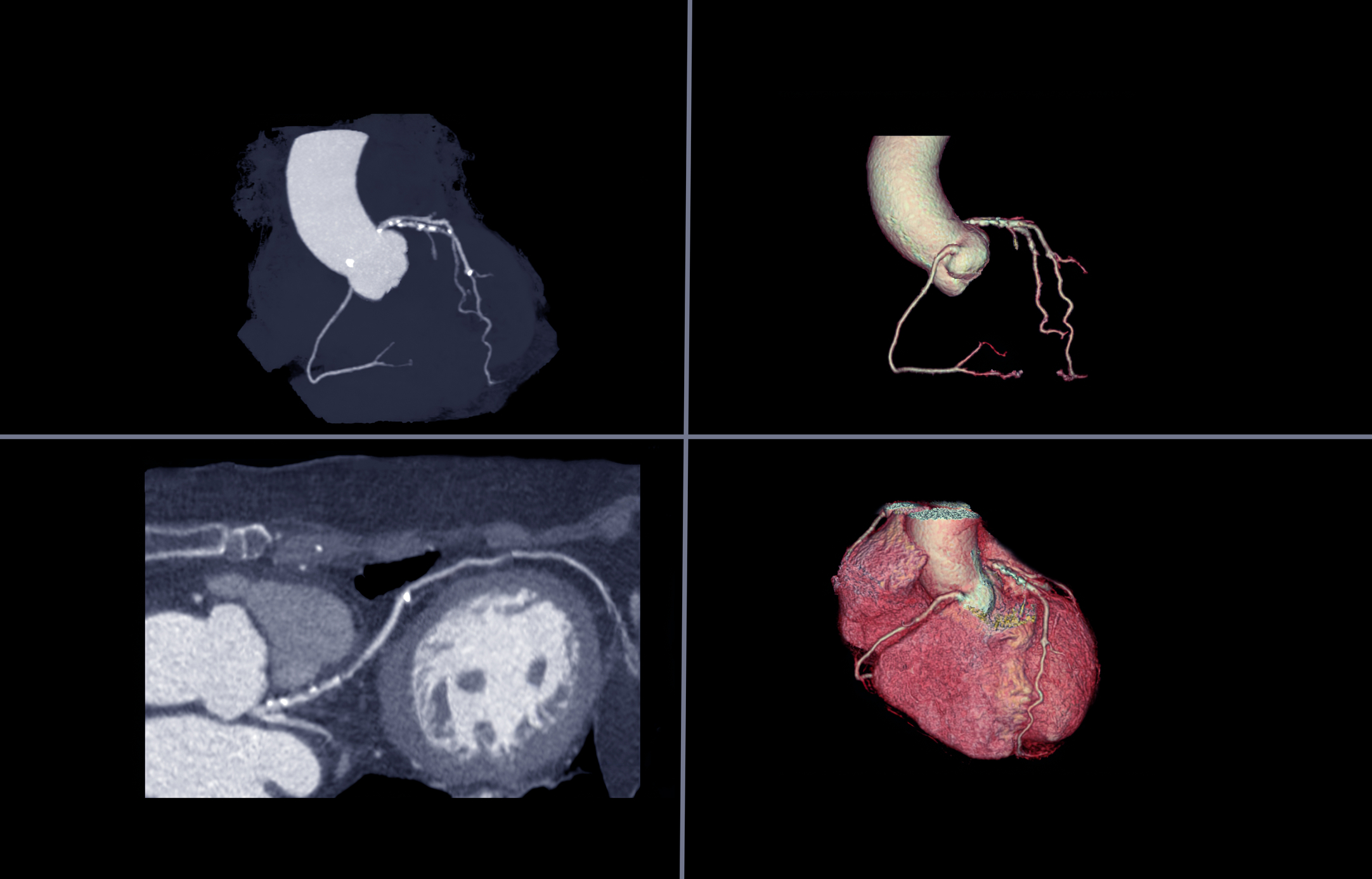
Computed Tomography Coronary Angiogram (CTCA) is a diagnostic imaging technique to evaluate coronary arteries. Computed tomography, known as a CT scan, utilises X-rays to produce cross-sectional images of the human body. Cardiac CT is an imaging technique that uses CT technology to visualise heart anatomy, coronary circulation, the aorta, pulmonary veins and arteries.
FACT: Cardiovascular diseases are the leading cause of death and account for 17.9 million lives globally each year, and 52.5% is contributed to coronary heart disease.
The primary function of the coronary arteries is to supply blood to the heart muscle. Therefore, the patient would require an injection of a contrast medium to image the arteries to show the blood vessels. Other diagnostic tests for coronary heart disease include invasive coronary angiography and non-invasive computed tomography (CT) coronary angiography.
CTCA imaging has revolutionised how physicians detect coronary artery disease due to its exceptional sensitivity.
Also, advancements in CTCA scanners in the clinical setting include increased gantry spin times and fast single-heartbeat scanning to improve image resolution and, most importantly, reduce the patient’s radiation exposure. Furthermore, developing specific algorithms has improved multidetector technology to facilitate scanning the entire heart volume in a single beat. These new CT coronary angiography scanners contain detector rows to enable 256 and 320-slice images to perform coverage of the whole heart in a single acquisition. This was possible by increasing the gantry spin times, which reduced the time for one rotation of an X-ray tube. The addition of a second X-ray tube further reduced the gantry spin times.
To limit unnecessary invasive coronary angiography on patients, the best approach would be to use at least a 64-slice CTCA scanner to rule out patients’ obstructive coronary stenoses and possibly coronary heart disease.
The advantage of these CTCA techniques is that the X-ray tube is only on for a short time, reducing stitching artefacts during acquiring the whole image in one sequence.
Today, the leading CT vendors have incorporated technology to scan the entire heart volume in a single beat. Another important factor when carrying out a CTCA is for the patient not to have a high heart rate and keep the effective radiation dose down. For example, the effective radiation dose given to a patient doubles when their heart rate increases from 55 to 60 beats per minute.
The Impact of the SCOT-HEART Trial on Clinical Decision-Making in Cardiology
The SCOT-HEART investigation concluded that patients who undergo CTA, when referred to a cardiology clinic, resulted in a lower risk of death from coronary heart disease. Also, patients benefited from CTCA from not having long-term use of invasive coronary angiography.
In the clinical setting, several types of CT scans can be used to diagnose heart disease, including calcium-score screening heart scan, coronary CT angiography (CTA) and total body CT scan.
Recent advances in CTCA include:
- Coronary artery calcium scoring (CACS) is used with stratification algorithms to assess risk.
- Development of CT-derived fractional flow reserve (FFR).
- Understanding plaque morphology and plaque characteristics.
- Development of machine learning (ML).
Coronary Artery Calcium Score (CACS)
Atherosclerosis results from coronary plaque leading to inflammation of the arterial intima, which leads to several heart diseases. However, the amount of coronary calcium can be used to predict any future heart problems, enabling the patient to make any necessary lifestyle changes to reduce their risk. For example, plaque formation can result from the calcification of the artery and the calcium score will estimate the extent of coronary artery disease. The calcium score considers the density of calcified coronary plaques in the coronary arteries.
The Agatston score can be used to quantify the level of calcification
Furthermore, if calcium is not present during the CTCA scan, it does not mean that you do not have any form of coronary disease. In some cases, soft plaque atherosclerosis could be present, which cannot be detected during a CT scan.
Fractional Flow Reserve (FFR): A Modern Approach to Assessing Coronary Artery Disease
Fractional Flow Reserve – Computed Tomography (FFR-CT) uses computational fluid dynamics to predict the functional significance of coronary artery lesions. It is a non-invasive procedure that uses HeartFlow® Analysis to provide the physician with a 3-D model of the coronary arteries to determine any potential blockages.
These blockages are generally due to coronary artery disease (CAD), which results from the arteries leading to the heart becoming narrow or blocked (atherosclerosis). This reduces blood flow to the heart, possibly leading to a heart attack.
The data obtained from a standard CTCA are further analysed using the coronary tree with CT-derived FFR results reported in all coronary segments. However, combining an anatomical and functional test will lead to a more accurate diagnosis and prevent a heart attack. Furthermore, invasive FFR is a well-established technique for quantifying lesion-specific ischaemia comparable to functional imaging.
Fractional flow reserve (FFR) is limited to a few dedicated centres in the UK. However, as CT-derived FFR technology advances over the coming years, it is expected to become increasingly available across the NHS. This diagnostic FFR test could be used in approximately 40,000 patients annually, saving the NHS £9.1 million annually. Therefore, the future of CT-derived FFR will be in the diagnostic array.
Plaque Morphology and Cardiovascular Disease
Understanding plaque morphology in cardiovascular diseases is becoming more important with the ability to visualise the entire vessel using CTCA scanning. The advantage of assessing plaque is establishing its nature using CT imaging to identify vulnerable plaque and its risk of developing the acute coronary syndrome.
Empowering Cardiovascular Diagnostics with Machine Learning
Machine Learning (ML) applies computer-based algorithms to evaluate a decision based on the relationship between multiple variables. These algorithms are used in diagnostic imaging to analyse large data sets and extract the relevant data. Therefore, analysis of CTCA data sets can potentially improve diagnoses and predicate lesions. In addition, ML will quantify markers, including calcium scoring, liver Hounsfield units, and epicardial fat volumes.
Integrating ML into clinical settings will help in the risk prediction of the patient towards cardiovascular diseases. For example, ML-based fractional flow reserve has been demonstrated in predicting ischaemic lesions.
The Future of Non-Invasive Cardiology
Techniques using CT have improved non-invasive diagnostic cardiology significantly over the past decade. CT based on FFR is highly likely to become increasingly prevalent to increase the accuracy of patients requiring invasive assessment/revascularization. In addition, in the subset of patients with previous percutaneous coronary intervention, CT perfusion techniques are currently being investigated. The most significant role of CTCA is in a primary prevention setting. Adding a calcium score when using calculators (Astro-CHARM and MESA) will enhance the accuracy of coronary intervention.
Disclaimer
The content provided in this article is intended for informational and educational purposes only and should not be construed as medical advice, diagnosis, or treatment. While every effort has been made to ensure the accuracy and currency of the information presented, Open Medscience does not guarantee its completeness or suitability for any specific purpose.
Computed Tomography Coronary Angiography (CTCA) and related technologies discussed herein should be interpreted and applied by qualified healthcare professionals. The inclusion of studies, data, or clinical trials does not imply endorsement or recommendation by Open Medscience.
Readers are advised to consult their healthcare provider or a qualified medical professional for any concerns regarding their health, medical conditions, or imaging results. Open Medscience shall not be held liable for any direct or indirect harm arising from the use or misuse of the information provided in this article.
Any mention of commercial products or brand names is for illustrative purposes only and does not constitute an endorsement.