Fever of unknown origin (FUO) is a challenging clinical problem that often requires extensive investigation to identify the underlying cause. Defined traditionally as a fever exceeding 38.3 °C on several occasions lasting for more than three weeks without a diagnosis after one week of inpatient investigation, FUO remains a diagnostic puzzle in modern medicine. The emergence of fluorodeoxyglucose positron emission tomography combined with computed tomography (FDG PET-CT) has significantly improved the diagnostic approach to FUO, offering valuable insights into its aetiology and guiding further management. This blog article explores the role of FDG PET-CT in FUO, focusing on its positivity rates and the distribution of diagnostic categories uncovered by this imaging modality.
The Clinical Challenge of Fever of Unknown Origin
FUO encompasses a wide spectrum of diseases, ranging from infections and malignancies to inflammatory and miscellaneous conditions. Traditional diagnostic pathways rely on detailed clinical evaluation, laboratory tests, and conventional imaging such as chest radiography, ultrasound, and computed tomography. However, these approaches often fail to localise the source of fever, particularly in cases where the disease is metabolically active but structurally subtle.
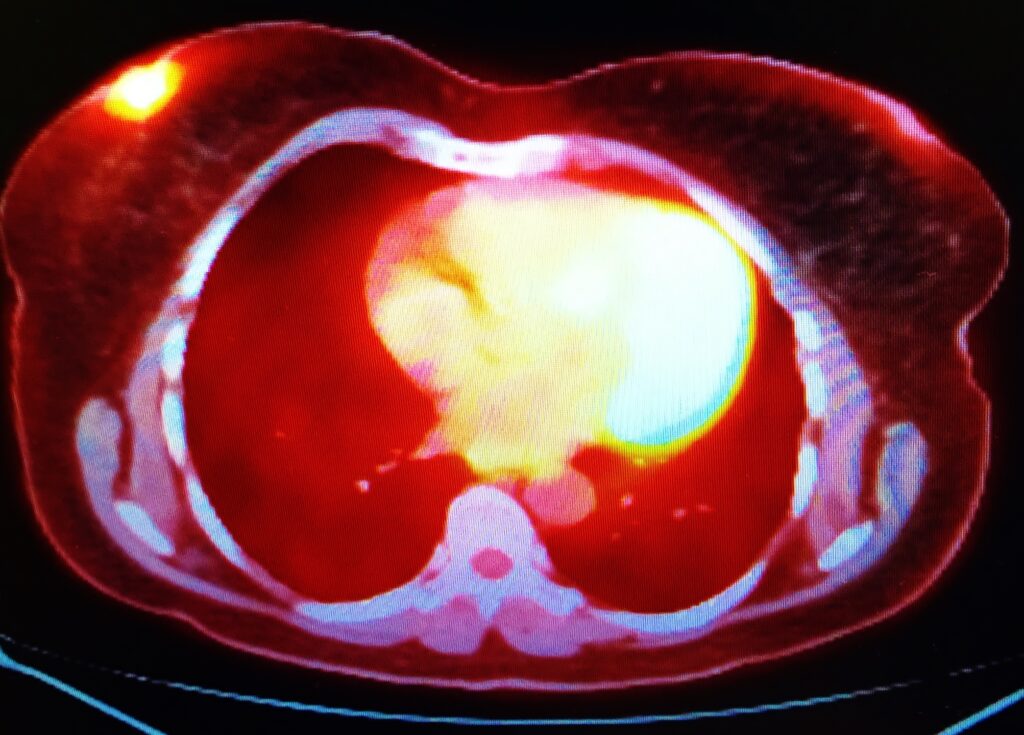
FDG PET-CT, which combines metabolic imaging with anatomical localisation, offers a unique advantage in this context. By detecting areas of increased glucose metabolism — a hallmark of infection, inflammation, and many cancers — FDG PET-CT can identify pathological processes that may not yet be anatomically apparent on conventional scans.
FDG PET-CT: Principles and Diagnostic Utility
The diagnostic strength of FDG PET-CT lies in its ability to highlight hypermetabolic tissue. Fluorodeoxyglucose (FDG), a glucose analogue labelled with fluorine-18, accumulates in cells with increased glycolytic activity. This includes activated leukocytes in infections and inflammatory diseases, as well as rapidly proliferating tumour cells. The PET component detects areas of FDG uptake, while the CT component provides precise anatomical localisation, enhancing specificity and aiding interpretation.
This dual capability makes FDG PET-CT a powerful tool in the evaluation of FUO, often detecting disease sites that were missed by other imaging modalities. Importantly, it can also guide targeted biopsies, reducing the need for blind sampling and invasive procedures.
Positivity Rates of FDG PET-CT in FUO
The effectiveness of FDG PET-CT in FUO is commonly assessed through its positivity rate — the proportion of scans that reveal clinically relevant findings leading to or contributing to a final diagnosis. Across multiple studies, FDG PET-CT demonstrates positivity rates ranging from 50% to 80%, with diagnostic yield varying depending on patient population, study design, and inclusion criteria.
Large retrospective analyses consistently show that FDG PET-CT contributes to establishing the diagnosis in more than half of FUO cases. For example, several multicentre studies report that approximately 55–70% of scans reveal findings that directly lead to a diagnosis or guide further targeted investigations. Even when FDG PET-CT does not yield a definitive diagnosis, it often identifies abnormalities that help narrow the differential diagnosis and direct clinical decision-making.
A key factor influencing positivity rates is the timing of PET-CT within the diagnostic pathway. Early use of FDG PET-CT tends to increase diagnostic yield, as it identifies active disease before it resolves spontaneously or becomes obscured by prior treatments such as antibiotics or corticosteroids. Conversely, delayed imaging may lead to false-negative results if disease activity has subsided.
Diagnostic Categories in FUO and FDG PET-CT Findings
The causes of FUO traditionally fall into four broad categories: infections, non-infectious inflammatory diseases (NIIDs), malignancies, and miscellaneous or undiagnosed cases. FDG PET-CT plays a role in identifying conditions across all these categories, with variable diagnostic performance depending on the underlying pathology.
Infections
Infectious causes account for a significant proportion of FUO cases, and FDG PET-CT is particularly useful in detecting occult infections that may not be evident on standard imaging. These include vascular infections such as endocarditis or mycotic aneurysms, deep-seated abscesses, vertebral osteomyelitis, prosthetic joint infections, and infections involving implanted medical devices.
Studies indicate that FDG PET-CT identifies infectious causes in approximately 20–40% of FUO cases. Its sensitivity is especially high for detecting infections involving metabolically active tissue and low-grade or chronic infections that produce subtle structural changes. However, specificity can be a limitation, as FDG uptake occurs in both infection and sterile inflammation. Correlation with clinical and laboratory findings remains essential for accurate interpretation.
Non-Infectious Inflammatory Diseases
NIIDs, including vasculitis, connective tissue diseases, and granulomatous conditions such as sarcoidosis, represent another major category of FUO. FDG PET-CT is particularly valuable for detecting large-vessel vasculitis, where increased FDG uptake along arterial walls can reveal disease even before anatomical changes are apparent on CT or MRI.
Positivity rates for NIIDs in the FUO series range from 15% to 30%. FDG PET-CT findings frequently lead to early diagnosis and initiation of immunosuppressive therapy, which can be crucial for preventing complications. In sarcoidosis and other granulomatous diseases, PET-CT can reveal widespread metabolic activity in lymph nodes, lungs, liver, or spleen, guiding biopsy to the most active sites and increasing diagnostic yield.
Malignancies
Malignant causes of FUO, though less common than infections or NIIDs, remain clinically important. Lymphomas, particularly non-Hodgkin and Hodgkin subtypes, are the most frequent neoplastic causes. FDG PET-CT excels in detecting metabolically active lymphomas, often revealing disease in nodes or extranodal sites that appear normal on conventional imaging.
The positivity rate for malignancy in FUO varies between 10% and 25% in published series. PET-CT is highly sensitive for lymphoma, but its specificity for malignancy is lower due to overlapping uptake patterns with inflammatory conditions. Therefore, histological confirmation remains necessary. Nevertheless, by pinpointing suspicious sites, FDG PET-CT reduces diagnostic delay and facilitates appropriate tissue sampling.
Miscellaneous and Undiagnosed Cases
A proportion of FUO cases remain unexplained even after exhaustive investigation, including FDG PET-CT. These cases, typically accounting for 10–20% of patients, may include rare conditions, drug-induced fevers, or spontaneously resolving febrile syndromes. In some instances, PET-CT findings are non-specific or incidental, requiring cautious interpretation to avoid misdiagnosis.
Importantly, a negative FDG PET-CT does not exclude serious disease but does carry prognostic value. Several studies suggest that patients with negative scans tend to have more benign courses, and many experience spontaneous resolution without long-term sequelae.
Factors Influencing FDG PET-CT Positivity and Interpretation
Several factors affect the diagnostic yield of FDG PET-CT in FUO. Patient preparation, such as adequate fasting and optimal blood glucose control, is essential to reduce background uptake and improve lesion detectability. Medications, particularly corticosteroids, can suppress metabolic activity and lead to false-negative results if administered before imaging.
Interpreting FDG PET-CT in FUO requires experience and clinical context. Not all areas of increased uptake are pathological; physiological uptake in brown fat, muscles, bowel, or urinary tract can mimic disease. Similarly, post-surgical inflammation and healing tissue can show FDG avidity. Multidisciplinary discussion incorporating clinical data, laboratory results, and imaging findings is often necessary for accurate diagnosis.
Clinical Impact and Future Directions
The integration of FDG PET-CT into the diagnostic pathway for FUO has transformed clinical practice. Its ability to identify metabolically active disease across diverse pathological categories significantly reduces diagnostic delay, guides targeted investigations, and informs therapeutic decisions. Early incorporation of FDG PET-CT is increasingly recommended in diagnostic algorithms, particularly when conventional investigations are inconclusive.
Ongoing research aims to refine PET imaging techniques, including the use of more specific tracers and hybrid imaging with PET/MRI, which may further enhance diagnostic accuracy and tissue characterisation. Advances in artificial intelligence and quantitative analysis may also improve lesion detection and interpretation, supporting more precise and personalised diagnostic strategies.
Conclusion
FDG PET-CT has become a cornerstone in the evaluation of fever of unknown origin, offering high positivity rates and valuable diagnostic insights across infections, non-infectious inflammatory diseases, malignancies, and other conditions. Its metabolic sensitivity allows detection of active disease even when structural changes are minimal, guiding further diagnostic steps and improving patient outcomes. While interpretation must be integrated with clinical context, the contribution of FDG PET-CT to the modern diagnostic work-up of FUO is undeniable. As imaging technology continues to evolve, its role is likely to expand further, enhancing the clinician’s ability to resolve one of medicine’s most persistent diagnostic challenges.
Disclaimer
The information provided in this article is intended for educational and informational purposes only and should not be interpreted as medical advice. FDG PET-CT is a diagnostic tool that must be used in conjunction with comprehensive clinical assessment, laboratory investigations, and other imaging modalities. Interpretation of PET-CT findings requires expert medical training and should always be performed by qualified healthcare professionals within the context of the patient’s overall clinical presentation. Although FDG PET-CT can significantly aid in the evaluation of fever of unknown origin, it does not replace the need for a thorough diagnostic work-up, and a negative scan does not exclude the presence of disease. Open MedScience does not accept any responsibility for decisions made based solely on the information contained herein. Patients should always seek personalised medical advice from their physician or specialist before undergoing any diagnostic procedure or treatment.
home » blog » nuclear medicine imaging »