Optimizing BTK Inhibitor Therapy: Insights from the ALPINE Zanubrutinib Trial
 By
By
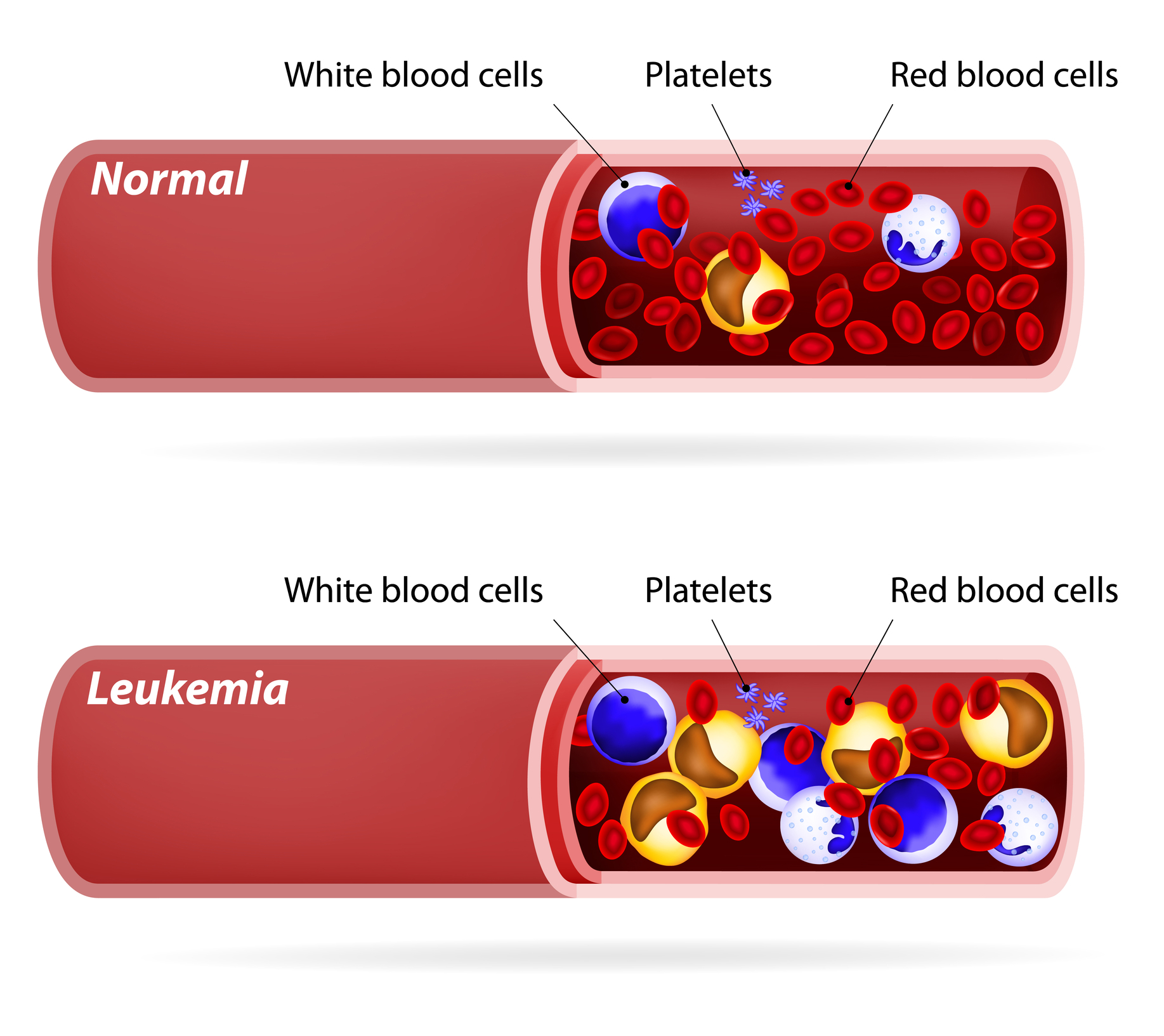
Discover the results of the ALPINE zanubrutinib trial, which showcases the effectiveness of new BTK inhibitors for CLL and SLL.
By
Discover the results of the ALPINE zanubrutinib trial, which showcases the effectiveness of new BTK inhibitors for CLL and SLL.
 By
By
Discover how specialty infusion care can provide effective treatments quickly, empowering patients in their health journey.
 By
By
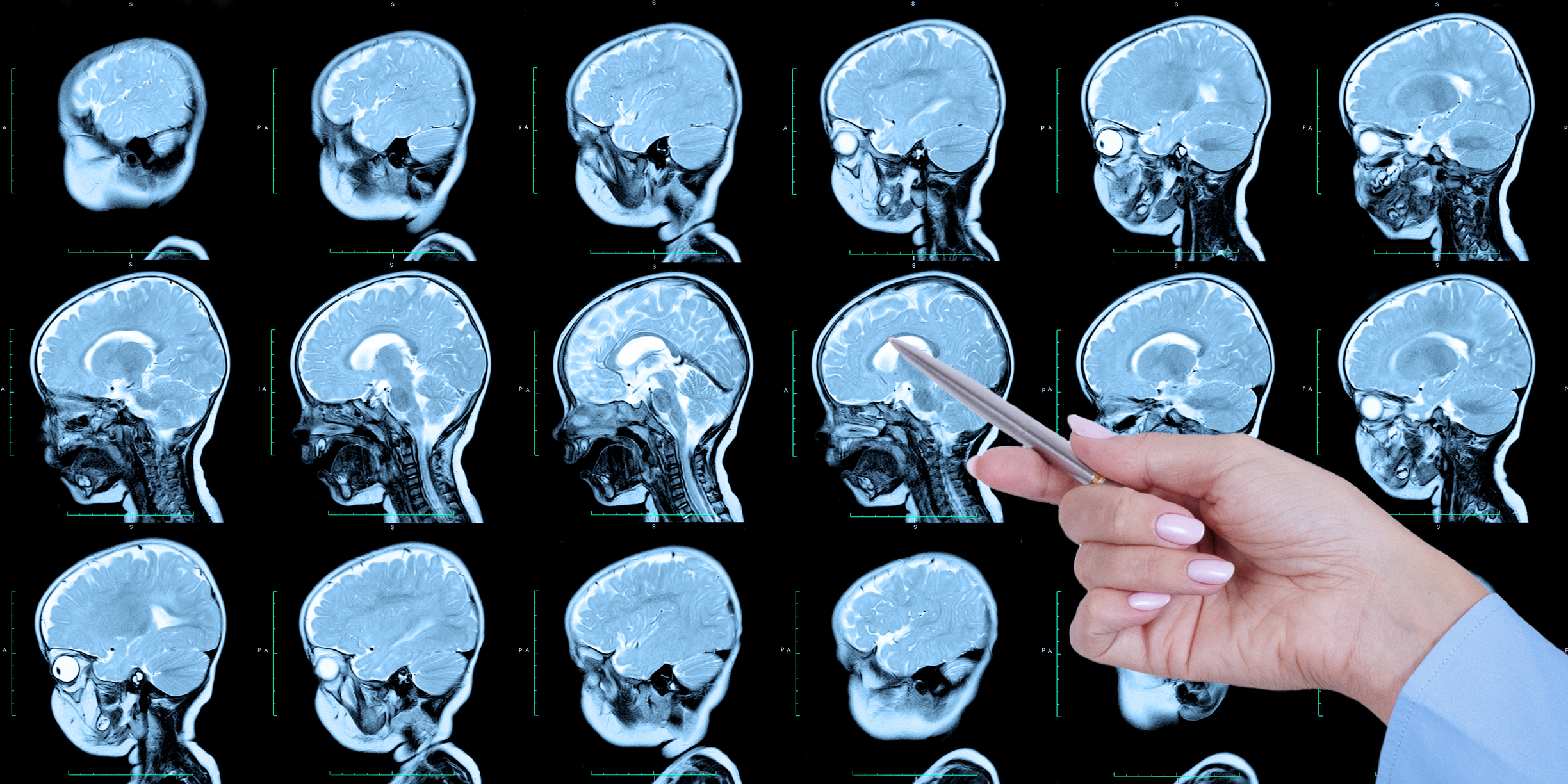
Explore the impact of oncology imaging errors on diagnosis and treatment outcomes in cancer care today.
 By
By
Understand how the oral microbiome and systemic inflammation are connected. Learn how mouth health influences diseases.
 By
By
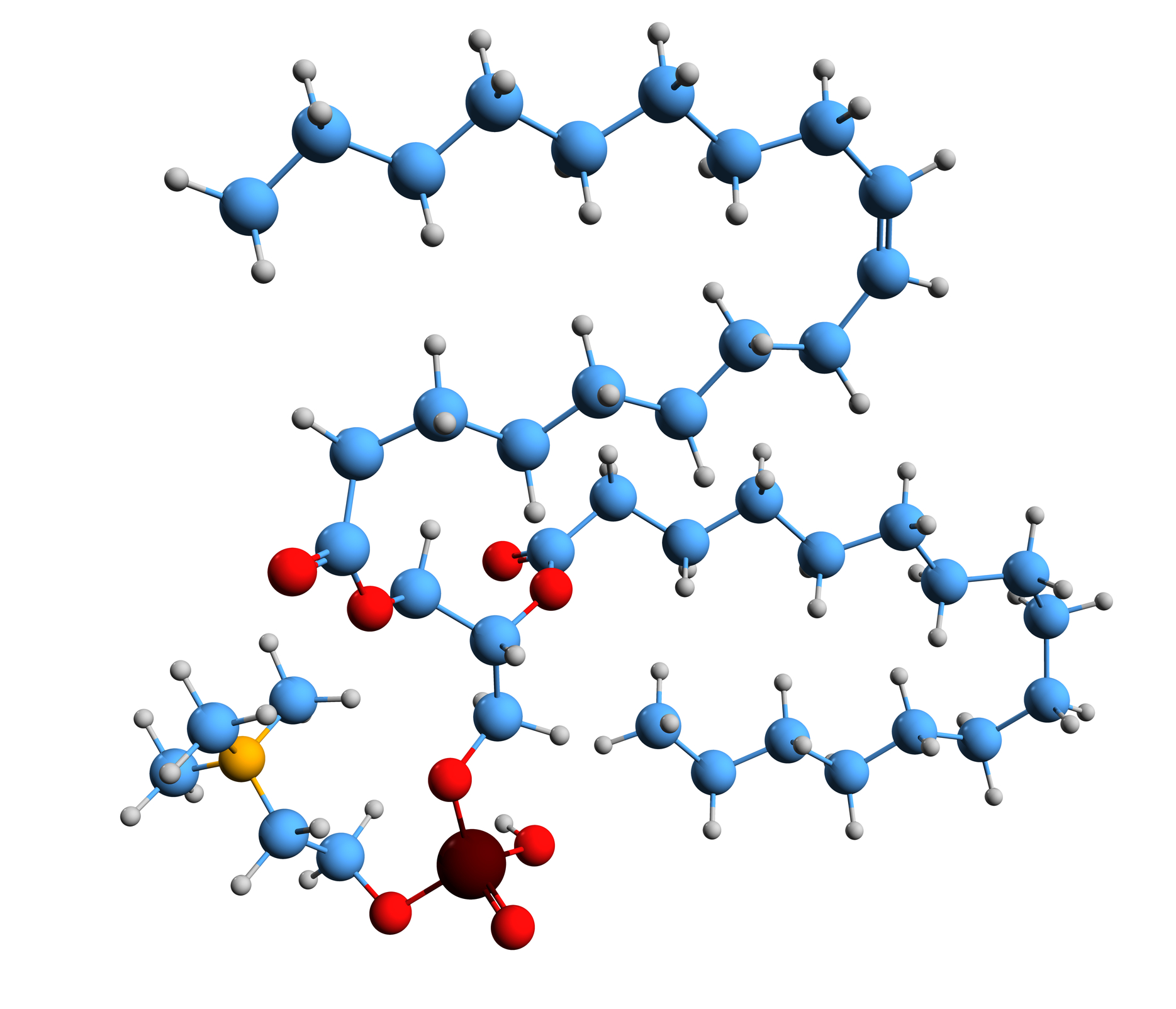
Discover how Palmitoyl Tripeptide-1 enhances tissue remodelling and cellular processes in this informative article.
 By
By
Discover how microfluidization in vaccine development enhances formulation quality and speeds up vaccine prototyping.
 By
By
Discover how experimental treatments legal disputes arise when cutting-edge therapies meet traditional malpractice law challenges.
 By
By
Relative dosimetry in radiation therapy enables precise measurement of dose distribution for effective and safe treatment delivery.
 By
By
Electron Beam Treatment Planning delivers precise, shallow-dose radiation, ideal for targeting superficial tumours while sparing deeper tissues.
 By
By
Learn about Chronic Lymphocytic Leukemia, a common cancer in adults, and how it affects the body and health over time.
 By
By
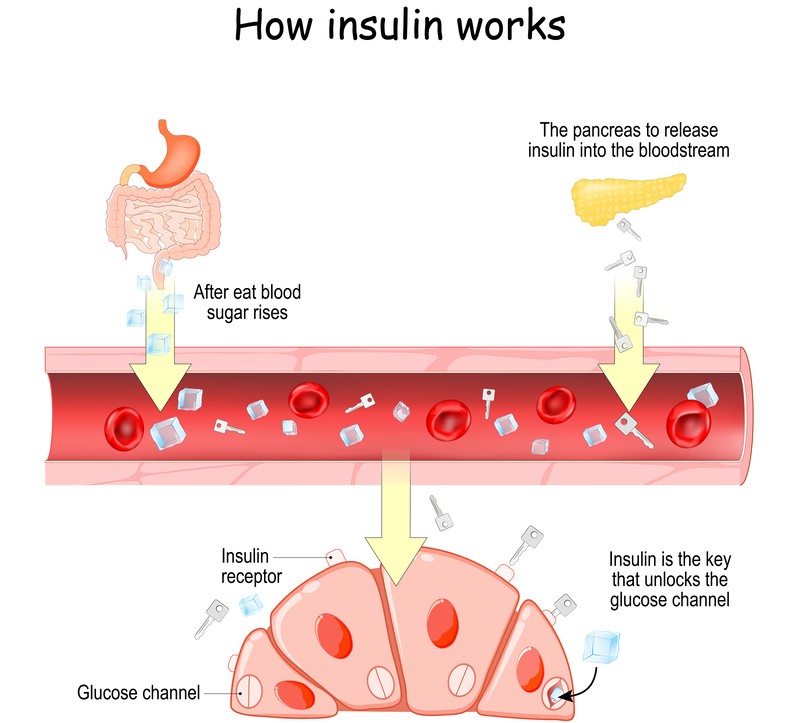
Pancreas plays a central role in digestion and metabolism by producing essential enzymes and hormones for bodily regulation.
 By
By
Best Dermatologist in Austin, TX provides comprehensive skin care, specialising in acne treatment, cosmetic procedures, and skin cancer screenings.
 By
By
Radiation therapy support significantly improves patient well-being, addressing physical symptoms, emotional needs, and enhancing treatment outcomes. Image for illustration only. Person depicted is a model.
 By
By
Robotic-assisted biopsy significantly enhances precision, enabling earlier lung cancer diagnosis and improving patient treatment outcomes effectively.
 By
By
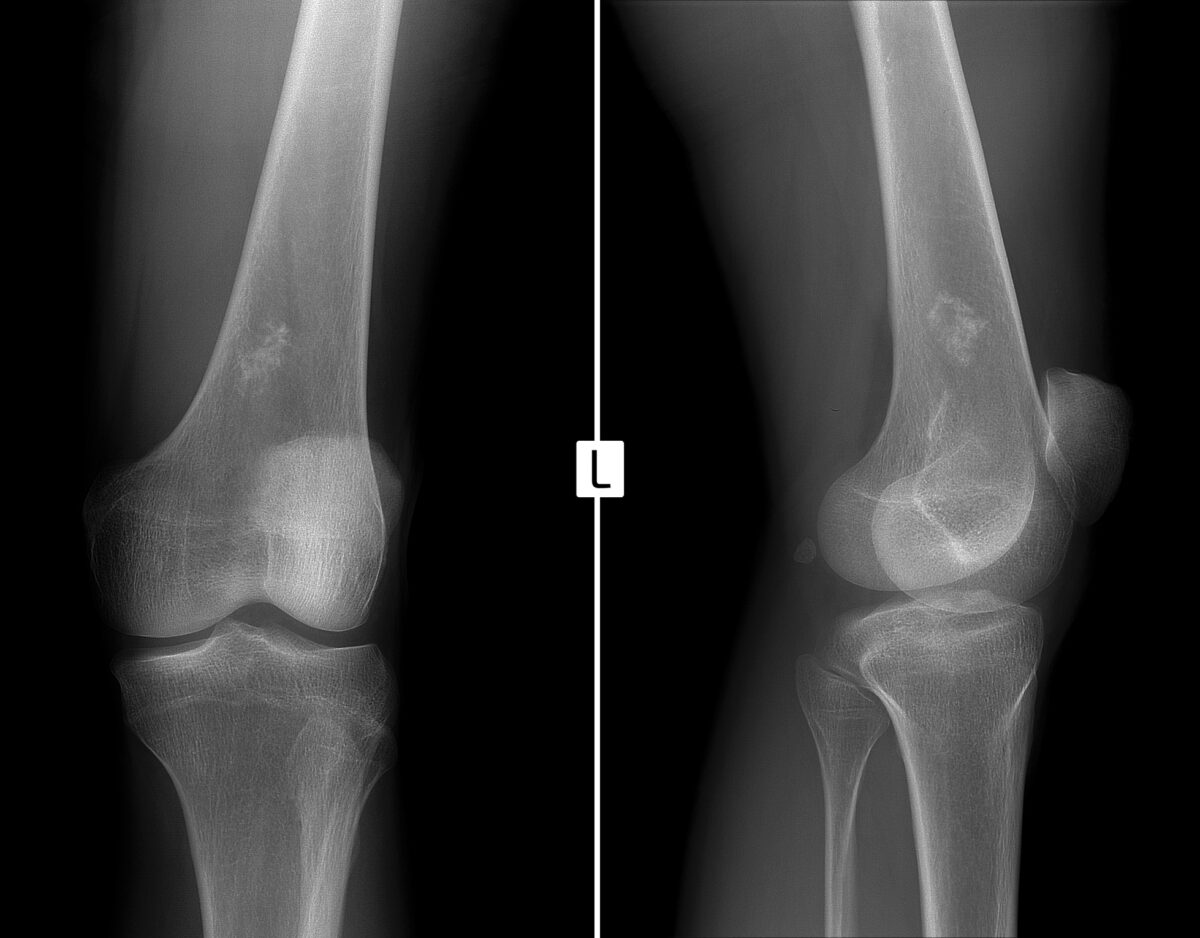
Yttrium-90 Tabituximab barzuxetan is a radiolabelled drug designed for targeted synovial sarcoma treatment.
 By
By
Yttrium-90 FAPi-46 targets fibroblast activation protein, providing effective radiotherapy for tumours and fibrotic diseases.
 By
By
Yttrium-90 FAPi-04 is a promising radiotherapeutic targeting fibroblast activation protein in cancer-associated fibroblasts effectively.
 By
By
Yttrium-90 Basiliximab combines targeted immunotherapy and radiotherapy, selectively attacking CD25-positive tumours with high therapeutic precision.
 By
By
Yttrium-90 Anditixafortide targets CXCR4-expressing tumours, delivering therapeutic β– radiation precisely, improving treatment outcomes significantly.
 By
By
Rhenium-SCT®: Innovative, precise, non-surgical therapy for non-melanoma skin cancer, ensuring safe and effective outcomes.
 By
By
RADIOPHARMACEUTICAL INNOVATION merges cutting-edge radiochemistry, targeted biology, and global clinical expertise, enhancing personalised treatments in oncology.
 By
By
Rhenium-188 HDD/Lipiodol therapy offers targeted radiopharmaceutical treatment for advanced hepatocellular carcinoma with portal vein thrombosis.
 By
By
Rhenium-188 P2045 is a peptide-based radiopharmaceutical targeting somatostatin receptors for treating neuroendocrine and pancreatic cancers.
 By
By
Lead-203 DOTA-VMT-MCR1 binds MC1R with high specificity, facilitating targeted imaging and image-guided therapy for metastatic melanoma patients.
 By
By
Nutraceuticals for health combine nature and science to enhance immunity, support digestion, and promote long-term wellness.
 By
By
Lutetium-177 MVT-1075 radioimmunotherapy targets pancreatic cancer by utilising CA19-9 specificity, sialyl-Lewis a binding, and precision radiation delivery.
 By
By
Advanced dermatological imaging provides detailed insights into skin layers, enhancing early disease detection, treatment accuracy, and overall patient care significantly.
 By
By
Lung function involves oxygen exchange, carbon dioxide removal, and maintaining optimal respiratory efficiency for overall bodily health. Image for illustration only. Person depicted is a model.
 By
By
Genomic research revolutionises healthcare by providing insights into diseases, enabling precise treatments, and improving patient outcomes worldwide.
 By
By
A novel radiolabelled drug, Lutetium-177 LNC1004, targets fibroblast activation protein, transforming cancer therapy through precision and innovation.